Outpatient Laparoscopic Cholecystectomy: Initial Results
Anuncio

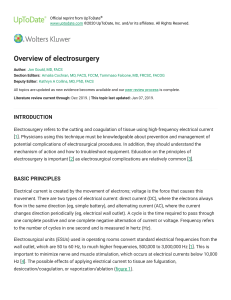
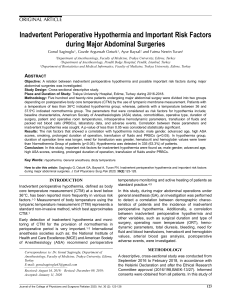
Original Articles Outpatient Laparoscopic Cholecystectomy: Initial Results of a Series of 200 Cases Francisco Martínez Ródenas, Raquel Hernández Borlán, Yaima Guerrero de la Rosa, José Moreno Solorzano, Ana Alcaide Garriga, Edmon Pou Sanchís, Gema Torres Soberano, José María Vila Plana, Jorge Pie García, and José Ramón Llopart López Badalona Serveis Assistencials, Hospital Municipal, Badalona, Barcelona, Spain Abstract Introduction. Outpatient laparoscopic cholecystectomy (CL) has not been generalised due to the fear of complications by the surgeon and preference of patients for hospitalisation. This situation could be changed by setting up strict selection criteria and providing hospital home care. The aims of this study are to find out what percentage of our population fulfil these criteria, confirm their validity and find out if the surgical process should be improved before being introduced. Material and method. A retrospective analysis was carried out on the first 200 elective CL cases dating from January 2006. The exclusion criteria were as follows: pre-operative criteria (social causes, age ⱖ70 years, unstable ASA III or ASA IV, an associated pathology or admission due to biliopancreatic pathology), intra-operative criteria (conversion, surgical time lasting longer than 90 minutes, non-identification or bleeding of the cystic artery, application of haemostatic material, haemorrhaging in the entrance ports, intra-abdominal bile spillage, drainage, difficulties in removing the gallbladder, anaesthetic and/or surgical complications) and post-operative (haemodynamic instability, excessive pain, nausea, and /or vomiting). Results. Out of the 200 cases, 53 (26.5%) patients fulfilled the criteria.The outpatient system was preferred predominantly by females and by those younger in age. Post-operative incidents occurred in 9.4% of the cases and these were dealt with by the hospital home care team. Conclusions. Ambulatory CL procedure is safe. Patients of advanced age or with associated pathologies Correspondence: Dr. F. Martínez Ródenas. BSA-Hospital Municipal. Vía Augusta, 9-13. 08911 Badalona. Barcelona. España. E-mail: [email protected] Manuscript received April 2, 2008; accepted for publication June 6, 2008. 262 Cir Esp. 2008;84(5):262-6 limit the inclusion. Hospital home care can solve any possible complications and contribute to the speedy discharge in those patients without criteria. Key words: Cholelithiasis. Outpatient laparoscopic cholecystectomy. Major ambulatory surgery. Hospital home care. COLECISTECTOMÍA LAPAROSCÓPICA AMBULATORIA: RESULTADOS INICIALES DE UNA SERIE DE 200 CASOS Introducción. La colecistectomía laparoscópica (CL) ambulatoria no se ha generalizado por temor del cirujano a las potenciales complicaciones postoperatorias y preferencia del paciente a la hospitalización. El establecimiento de criterios selectivos estrictos y la hospitalización a domicilio podrían cambiar esta predisposición. Los objetivos de este estudio son averiguar qué porcentaje de nuestra población con colelitiasis cumple dichos criterios, confirmar su validez y descubrir si debe mejorarse el proceso quirúrgico antes de implementarse. Material y método. Se analizan prospectivamente los primeros 200 casos de CL electiva desde enero de 2006. Los criterios de exclusión son: preoperatorios (causas sociales, edad ⱖ 70 años, ASA III inestable o ASA IV, enfermedad concomitante que precisa control hospitalario, ingreso previo por afección biliopancreática), intraoperatorios (conversión a laparotomía, tiempo quirúrgico ⱖ 90 min, sin identificación o sangrado de la arteria cística, aplicación de material hemostático, hemorragia en puertas de entrada, vertido de bilis intraabdominal, drenajes, extracción dificultosa de vesícula, complicaciones anestésicas y/o quirúrgicas) y postoperatorios (inestabilidad hemodinámica, dolor excesivo, náuseas y/o vómitos en la sala de reanimación). Resultados. Cumplieron criterios 53 (26,5%) pacientes. El sexo femenino y la menor edad favorecen Martínez Ródenas F et al. Outpatient Laparoscopic Cholecystectomy: Initial Results of a Series of 200 Cases el proceso ambulatorio. Se presentaron incidencias postoperatorias en el 9,4% que podrían asumirse por el equipo de hospitalización a domicilio. Conclusiones. La CL en régimen ambulatorio es segura. La edad avanzada y la enfermedad concomitante limitan la inclusión. La hospitalización a domicilio puede solucionar las posibles complicaciones y facilitar el alta precoz de los pacientes sin criterios de CL ambulatoria. Palabras clave: Colelitiasis. Colecistectomía laparoscópica ambulatoria. Cirugía mayor ambulatoria. Hospitalización a domicilio. Introduction In the 1990s, outpatient laparoscopic cholecystectomy (LC) safety and ability to reduce hospital costs were described and demonstrated.1,2,3 However, despite being performed in several hospitals in Spain,4-6 this procedure is not widelyused in this country.This is primarily because of the possibility of postoperative complications, doubt on the part of the surgeon of the availability of a safe backup to assume responsibility7 and patient preference for hospitalisation.8 Because of this, the majority of cases are hospitalised for a minimum of 1 night.9 The availability of a home care unit in our hospital, which makes it possible to have 24-hour telephone consultation and surgeon and nursing house calls in the first days following surgery, provides us with the ability to evaluate the possibility of performing this operation on a major ambulatory surgery basis for cases that meet certain criteria. The objectives proposed for this study have been: – To study what percentage of our population with symptomatic cholecystitis met the criteria for outpatient LC – To confirm if the selection criteria were adequate – To study the causes for exclusion among potential candidates – To validate the safety of outpatient LC – To identify potential areas for improvement in case of adverse clinical results Material and Method Study Design and Subjects Prospective and observational clinical study performed between January 2006 and August 2007 at BSA-Hospital Municipal. The first 200 patients who underwent elective LC for cholelithiasis were included. All surgeons in the department participated in the operations. LC was performed under balanced general anaesthesia in the French position with a Hasson trocar and two 5 and 10 mm accessory trocars. A fourth trocar was used for cases of difficult Calot’s triangle exposure. The abdominal cavity was insufflated with CO2 at an intra-abdominal pressure <14 mm Hg and gastric decompression was performed in cases of gastric distension. Selection guidelines were used of antibiotic prophylaxis (age >65 years, history of acute cholecystitis, pancreatitis or jaundice and bile spillage into the abdominal cavity) and for perioperative cholangiography (history of jaundice or pancreatitis, bilirubin or alkaline phosphatase changes and dilation of the common bile duct >6 mm by ultrasound). The patients were seen in outpatient surgery consultation at 1 month after discharge and a general follow-up panel with liver function testing was performed on those patients who had persistent symptoms. Exclusion Criteria for Outpatient LC The exclusion criteria have been chosen from criteria used by other authors.1,10-15 and have been classified as preoperative, intraoperative, and postoperative. – Preoperative exclusion criteria: social causes (lack of family support, lack of telephone, living far from the hospital), age ≥70 years, unstable ASA III or ASA IV, concomitant disease that requires hospital monitoring, obesity (body mass index ≥35) and prior admission for a biliopancreatic condition (acute cholecystitis, pancreatitis, and obstructive jaundice) – Intraoperative exclusion criteria: conversion to laparotomy, surgical time >90 minutes, lack of identification of the cystic artery or haemorrhage, use of haemostatic material in the liver bed, haemorrhage in the entrance ports, intra-abdominal bile spillage, placement of a drain, difficult extraction of the gallbladder through the umbilical incision, anaesthesia complications and surgical complications – Postoperative exclusion criteria (recovery room): haemodynamic instability, excessive pain on the visual analogue scale (VAS) and poorly controlled nausea and/or vomiting The VAS quantitative model was used to evaluate postoperative pain. It consists of a diagram with a 10 cm long horizontal line where the ends are marked with the expressions “no pain” and “maximum pain imaginable.” The patient marks the pain intensity on the line relative to the ends. Pain was considered to be excessive when the distance measured from the “no pain” end to the mark was greater than 3 cm. Analysis of the Data The results obtained have been analysed statistically using the STATWIEW 512+ programme for the Macintosh personal computer. The χ2 independence test was used for comparison of quantitative variables and analysis of variance between qualitative and quantitative variables. A P value less than .05 was considred significant.The results are expressed as the median (standard deviation). Results Hundred forty-one women and 59 men underwent surgery, with a median age of 57.3 (15.1) (range, 20-85) years. Overall morbidity in the study was 8.5%. This occurred during hospitalisation in 6 patients (1 biliary leak, 2 cases of acute urinary retention, 2 trocar bleeds, and 1 wound infection). One patient had a subhepatic abscess at followup that required reintervention, another had a subhepatic collection that was treated conservatively and there were 3 wound infections. There was no mortality. The rate of conversion to laparotomy was 5.5%. Hospital stay was 2.1 (0.9) days. Eighty-one (40.5%) patients met the preoperative inclusion criteria, with important differences with regards to gender (65 women vs 16 men; P<.05) (Figure 1). Causes for preoperative exclusion are shown in Figure 2. The most significant criteria for intraoperative exclusion was intra-abdominal bile spillage of any amount with or without calculi during dissection of the gallbladder off the liver bed, which occurred in 19 (23.5%) of the 81 patients included. Extraction of the gallbladder through the umbilical incision was difficult on 2 occasions in this subgroup. Of the remaining 8 patients 2 were excluded, 3 were due to placement of an abdominal drain, 3 due to use of haemostatic material, 1 due to intestinal puncture, and 1 due to a surgery time greater than 90 minutes. Cir Esp. 2008;84(5):262-6 263 Martínez Ródenas F et al. Outpatient Laparoscopic Cholecystectomy: Initial Results of a Series of 200 Cases Relationship Between Exclusion Criteria for Outpatient Laparoscopic Cholecystectomya Preoperative Criteria, % 200 Patients Preoperative Criteria 81 Included 40.5% (Total) 119 Excluded Intraoperative criteria, % Yes No Yes No 76.1 37.9 23.9 62.1 a P<.001. Intraoperative Criteria 54 Included 66.6% (Preoperative Criteria) 27% (Total) 27 Excluded Postoperative Criteria 53 Included 98.2% (Intraoperative Criteria) 26.5% (Total) 1 Excluded Figure 1. Patient distribution according to preoperative, intraoperative, and postoperative inclusion criteria met. Age (≥70 Years) 8 3 21 Prior Admission Cholecystitis Pancreatitis Obstructive Jaundice 11 28 10 38 Concomitant Disease Hypertension Diabetes Heart Disease Chronic Obstructive Pulmonary Disease Cirrhosis Cerebral-Vascular Accident Epilepsy Amaurosis Morbid Obesity Figure 2. Exclusion criteria for 119 patients without preoperative inclusion criteria. There is a good correlation between the preoperative and the intraoperative exclusion criteria (Table). In our study, 76.1% of patients who were excluded preoperatively also met intraoperative exclusion criteria. Following the operation, 264 Cir Esp. 2008;84(5):262-6 1 patient presented abdominal pain and haemodynamic instability during their stay in the recovery room. Therefore, hypothetically, 53 (26.5%) patients were discharged according to the outpatient LC programme (Figure 1). Patients who met all the criteria for outpatient LC were younger (43.8 [10.4] vs 62.2 [13.5] years; P<.001); the percentage of women was greater than men’s (31.9% vs 13.6%; P<.05). Five patients suffered incidents on the ward: vomiting (2), pain (1), both symptoms (1), and acute urinary retention (1) (morbidity was 1.9%). In theory, this means 9.3% of the 53 patients who were discharged suffered problems at home. Discussion Many authors consider LC and inguinal herniorrhaphy to be procedures that can be performed on an outpatient basis with better safety and efficacy.16,17 Nevertheless, though outpatient treatment for hernia has become common, outpatient LC is still far from common. This is due to the fact that these procedures are not comparable. In the case of LC, this situation is created by the risk for potential serious postoperative complications and uneasiness on the part of the surgeon to assume responsibility when faced with the lack of adequate home health services and due to legal uncertainties7,10,18,19; in addition to patient objections who, because of uneasiness, may assume that admission to hospital is the best option for treatment.8 Therefore, in order to ensure successful introduction of this project in our organisation, the following strategy has been employed: ascertain what percentage of the population would be affected, confirm the safety of the procedure in order to assure our patients and surgeons and study whether improvements should be made prior to being carried out. Currently, 26.5% of our reference population of patients with symptomatic gallstones may benefit from outpatient LC. This percentage, which may appear to be low when compared to other studies,12-15 is the result of very stringent selection criteria, the purpose of which, as stated above, is to confirm the safety of outpatient LC, to avoid rejection by patients and surgeons and to reinforce its success in our centre. Our results are closer to those published by Voyles et al,20 which revealed that only a third of 1750 patients evaluated in their institution met the selection criteria. The preoperative, intraoperative, and postoperative selection criteria chosen in our study are sufficient because Martínez Ródenas F et al. Outpatient Laparoscopic Cholecystectomy: Initial Results of a Series of 200 Cases those patients who meet all of the criteria have a minimal risk for and severity of postoperative incidents and morbidity. There is good correlation between the preoperative and intraoperative causes for exclusion; a preoperative cause for exclusion predicts that there will be an intraoperative cause 76.1% of the time. Therefore, from a practical point of view, the preoperative criteria are useful since they permit sufficient selection prior to surgery. These selection criteria may be relaxed in 2 given situations once outpatient LC is consolidated in our centre. Half of patients without concomitant disease and with a history of acute pancreatitis, and the majority of patients with intraabdominal bile spillage, met the postoperative criteria and would also have benefitted from the outpatient procedure. As with our findings, a recent study14 indicates that gallbladder perforation is not an intraoperative factor that predicts failure of the outpatient protocol. Apart from 1 patient who suffered urinary retention, the other postoperative incidents were related to pain, nausea, and/or vomiting. Before initiating the programme, establishing an analgesic and antiemetic protocol is a top priority in order to improve the quality of our results and to avoid the occurrence of these problems in the patient’s home. Postoperative nausea and vomiting are the main cause of unexpected hospital admission, which varies by study15,21 between 1% and 39%. Poorly-controlled postoperative pain, conversion to laparotomy and uneasiness on the part of the patient also contribute.15 The rate of readmission varies from 1.9% to 8% and is related to morbidity21; in which residual bile duct lithiasis is an important cause. Some authors have questioned the safety of outpatient cholecystectomy treatment.22,23 Nevertheless, some studies24,25 have shown that, with regards to vital complications (1/2000 LC), these become symptomatic within the first hours following surgery, so they would be detected during hospitalisation, and other complications, such as injury to the bile duct (0.3%-1%), are not usually discovered until the second day following surgery; as such, a 4-6 hour observation period would be prudent since hospital admission would not reduce detection of later major complications.15 After confirming the incidences of postoperative morbidity of the candidates who met the selection criteria, it can be stated that outpatient LC is a safe procedure in our area and that the minimal complications, should they appear, can be evaluated and resolved effectively by our home health team.This team may also facilitate early discharge for patients who did not meet the criteria needed for outpatient LC. Our results reveal that female gender and lower age are factors that facilitate outpatient LC. These results coincide with the findings reported by Lau et al.12 The success of a major ambulatory surgery programme depends on the effort and coordination between surgeons, anaesthesiologists and nursing staff. Sufficient information to the patient is fundamental in order to gain their trust and acceptance, as is understanding their opinion.26 There is no doubt that all of the activities developed in order to establish a major ambulatory surgery programme will result in an improvement in quality of care in addition to providing an economic benefit to the healthcare system.8,14,27,28 References 1. Reddick EJ, Olsen DO. Outpatient laparoscopic laser cholecystectomy. Am J Surg. 1990;160:485-7. 2. Arregui ME, Davis CJ, Arkush A, et al. In selected patients outpatient laparoscopic cholecystectomy is safe and significantly reduces hospitalization charges. Surg Laparosc Endosc. 1991;1:240-5. 3. Zegarra RF 2nd, Saba AK, Peschiera JL. Outpatient laparoscopic cholecystectomy: safe and cost effective? Surg Laparosc Endosc. 1997;7:487-90. 4. Pardo J, Ramia R, Martín JM, López A, Padilla D, Cubo T, et al. Colecistectomía laparoscópica ambulatoria. Cir Esp. 1998;64:37-9. 5. Serralta A, García R, Martínez P, Hoyas L, Planells M. Cuatro años de experiencia en colecistectomía laparoscópica ambulatoria. Rev Esp Enferm Dig. 2001;93:207-10. 6. Bermúdez I, López S, Sanmillán A, González C, Baamonde de la Torre I, Rodríguez A, et al. Colecistectomía laparoscópica en régimen ambularorio. Cir Esp. 2004;76:159-63. 7. Henderson J, Goldacre MJ, Griffith M, Simmons HM. Day-case surgery: geographical variation, trends, and readmissions rates. J Epidemiol Community Health. 1978;43:301-5. 8. Planells M, Sánchez A, Sanahuja A, Bueno J, Serralta A, García R, et al. Gestión de la calidad toral en colecistectomía laparoscópica. Calidad asistencial y calidad percibida en colecistectomía laparoscópica ambulatoria. Rev Esp Enferm Dig. 2002;94:319-25. 9. Turienzo EO, Rodríguez JI, Trelles A, Aza J. Gestión integral del proceso de colecistectomía laparoscópica. Cir Esp. 2006;80: 385-94. 10. Fiorillo M, Davidson P, Fiorillo M, D’Anna J, Sithian N, Silich R. 149 ambulatory laparoscopic cholecystectomies. Surg Endosc. 1996;10: 52-6. 11. Cuschieri A. Day-case (ambulatory) laparoscopic surgery: let us sing from the same hymn sheet. Surg Endosc. 1997;11:1143-4. 12. Lau H, Brooks DC. Transitions in laparoscopic cholecystectomy. The impact of ambulatory surgery. Surg Endosc. 2002;16:323-6. 13. Martínez A, Docobo F, Mena J, Durán I, Vázquez J, López F, et al. Colecistectomía laparoscópica en el tratamiento de la litiasis biliar: ¿cirugía mayor ambulatoria o corta estancia? Rev Esp Enferm Dig. 2004;96:452-9. 14. Bueno J, Planells M, Sanahuja A, García R, Arnau C, Guillemot M. Factores intraoperatorios predictivos del fracaso del régimen ambulatorio tras colecistectomía laparoscópica. Cir Esp. 2005;78:168-74. 15. Bueno J, Planells M, Arnau C, Sanahuja A, Oviedo M, García R, et al. Colecistectomía laparoscópica ambulatoria. ¿El nuevo “gold standard” de la colecistectomía? Rev Esp Enferm Dig. 2006;98: 14-24. 16. Campanelli G, Cavagnoli R, Cioffi U, de Simona M, Fabián M, Pietro P. Can laparoscopic cholecystectomy be a day surgery procedure. Hepatogastroenterology. 1998;45:1422-9. 17. Keulemans Y, Eshuis J, de Haes H, de Wit L, Gonma DI. Laparoscopic cholecystectomy: day-care versus clinical observation. Ann Surg. 1998;228:730-40. 18. Saunders CJ, Leary BF, Wolfe BM. Is outpatient laparoscopic cholecystectomy wise? Surg Endosc. 1997;11:1147-9. 19. Joshi GP, Twersky R. Fast tracking in ambulatory surgery. Amb Surg. 2000;8:185-90. 20. Voyles CR, Berch BR. Selection criteria for laparoscopic cholecystectomy in an ambulatory care setting. Surg Endosc. 1997; 11:1145-6. 21. Lau H, Brooks DC. Contemporary outcomes of ambulatory laparoscopic cholecystectomy in a major teaching hospital. World J Surg. 2002;26:1117-21. 22. Llorente J. Laparoscopic cholecystectomy in the ambulatory surgery setting. J Laparoendosc Surg. 1992;2:23-6. 23. Saunders C, Learvy B, Wolfe B. Is outpatient laparoscopic choleystectomy wise? Surg Endosc. 1995;9:1263-8. 24. Deziel D, Millikan K, Economou S, Doolas A, Ko S, Airan M. Complications of laparosocpic cholecystectomy: a nacional survey of 4,929 hospitals anda n análisis of 77,604 cases. Am J Surg. 1993;165: 9-14. 25. Richarson M, Bell G, Fullarton G. Incidente and nature of bile Duch injuries following laparosocpic cholecystectomy: an audit of 5913 cases.West of Scotland Laparoscopic Cholecystectomy Audit Group. Br J Surg. 1996;83:1356-60. 26. Codina J, Martínez-Ródenas F, Utrera C, Díaz L, Sánchez P, Pié P. La opinión del paciente en cirugía mayor ambulatoria y su inclusión como parámetro de calidad. Cir Esp. 1998;64:28-32. Cir Esp. 2008;84(5):262-6 265 Martínez Ródenas F et al. Outpatient Laparoscopic Cholecystectomy: Initial Results of a Series of 200 Cases 27. Keulemans Y, Eshuis J, de Haes H, De Wit LT, Gouma DJ. Laparoscopic cholecystectomy: day care versus clinical observation. Ann Surg. 1998;228:734-40. 266 Cir Esp. 2008;84(5):262-6 28. Lillemoe KD, Lin JW, Talamini MA, Yeo CJ, Synder DS, Parker SD. Laparoscopic cholecystectomy as a “true” outpatient procedure: initial experience in 130 consecutive patients. J Gastrointest Surg. 1999;3:44-9.