household application - Long Beach Unified School District
Anuncio

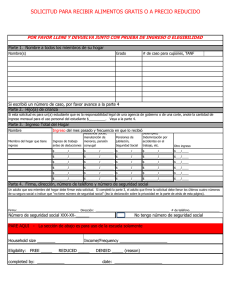
APPLICATION INSTRUCTION SHEET AND CHECK LIST HOUSEHOLD APPLICATION: COMPLETE THE APPLICATION SIDE OF THE FORM ONLY. DO NOT STAPLE OR DAMAGE. IF YOUR APPLICATION IS NOT COMPLETE, YOUR CHILD’S MEAL BENEFITS WILL BE DELAYED. USE THIS CHECKLIST TO MAKE SURE YOUR APPLICATION IS COMPLETE. For CalWORKs, CalFresh (formerly Food Stamps), KinGAP, or FDPIR Households: Section I: List all children in the household (whether they attend school or not). List the LBUSD school or LBUSD CDC program. Write in grade for 2015-2016 school year Check the box next to the type of benefit any family member receives. Write in the NAME AND CASE NUMBER of the individual receiving the benefits. Sign the application and date. If No One in your household gets CalWORKS, CalFresh, KinGAP, or FDPIR benefits: Section I & Section II: List all children in the household (whether they attend school or not). List the LBUSD school or LBUSD CDC program. Write in grade for 2015-2016 school year List any income received by a child from full-time or regular part-time employment or for SSI, Adoption Assistance or personal use income for a foster child. List all adults in the household with the INCOME AND FREQUENCY each adult receives before taxes or any other amount is taken out. If any adult listed has no income, check the “no income” box. • Make sure to list income of each adult in the correct column. List income and FREQUENCY of income received from all sources. Sign the application and date. Make sure to list the household member signing the application in the adult section and state his/her income in the appropriate column. List the last four digits of the social security number of the adult household member signing the application. If the adult who signs the application has no social security number, check the box “I do not have social security number.” FOSTER CHILDREN ARE TO BE LISTED WITH OTHER CHILDREN IN THE HOME AND COUNTED IN HOUSEHOLD SIZE. For Foster Child: Section I List all children in the household (whether they attend school or not). List the LBUSD school or LBUSD CDC program. Write in grade for 2015-2016 school year Check box in column for “Foster Child.” If all students are foster children, then skip to section III. If not all children in the household are foster children, complete all sections of the application that are applicable and list personal use income for each foster child in Section II. Sign the application and date. Completed applications for free and reduced-price meals may be returned to any open school site any time during a school day or the Nutrition Services Office (3333 Airport Way, Long Beach CA 90806). Does your child have special dietary needs? If so, call a Child Nutrition Specialist at (562) 427-7923. INSTRUCCIONES PARA LLENAR LA SOLICITUD Y LISTA DE VERIFICACIÓN SOLICITUD DEL HOGAR: COMPLETE SOLAMENTE EL LADO DE LA SOLICITUD. NO USE GRAPAS NI DAÑE EL FORMULARIO. SI NO COMPLETA LA SOLICITUD, LOS BENEFICIOS DE ALIMENTOS PARA SU NIÑO(A) SE DEMORARÁN. USE ESTA LISTA DE VERIFICACIÓN PARA COMPLETAR CORRECTAMENTE LA SOLICITUD. Para hogares de CalWORKs, CalFresh (conocido como Estampillas de Alimentos), KinGAP, o FDPIR: Sección I: Anote a todos los niños en el hogar (asistan o no a la escuela). Anote la escuela del LBUSD o un programa de CDC del LBUSD. Escriba el grado para el año escolar 2015-2016 Marque el casillero al lado del tipo de beneficio que recibe cualquier miembro de la familia. Escriba EL NOMBRE Y EL NUMERO DE CASO de la persona que recibe los beneficios. Firme la solicitud. Si nadie en su hogar recibe beneficios de CalWORKS, CalFresh, KinGAP, o FDPIR: Sección I y Sección II: Anote a todos los niños en el hogar (asistan o no a la escuela). Anote la escuela del LBUSD o un programa de CDC del LBUSD. Escriba el grado para el año escolar 2015-2016 Anote cualquier ingreso recibido por parte de hijo(a) que venga de un empleo de tiempo completo o empleo regular de tiempo parcial, o por SSI o Asistencia de Adopción o uso personal de ingresos por niños de crianza. Anote a todos los adultos en el hogar con sus ingresos antes de que se deduzcan los impuestos o cualquier otra CANTIDAD Y LA FRECUENCIA con que los reciben. Si un adulto no recibe ingresos, marque el casillero “NO hay ingresos”. Asegúrese de anotar el ingreso de cada adulto en la columna correcta. Anote el ingreso y la FRECUENCIA con que se recibe el ingreso de todas las fuentes de ingreso. Anote el ingreso que recibe un hijo(a) de un empleo normal de tiempo parcial o tiempo completo o de SSI, Asistencia de Adopción, o uso de ingreso personal por un niño de crianza. Firme la solicitud y escriba la fecha Anote el nombre del miembro de la familia que firma la solicitud en la sección de adultos e indique su ingreso en la columna apropiada. Anote los últimos 4 números del seguro social de la persona adulta que firma la solicitud. Si el adulto que firma la solicitud no tiene un número de seguro social, marque el casillero “No tengo número de seguro social.” LOS NIÑOS DE CRIANZA SE DEBEN INCLUIR JUNTO CON LOS OTROS NIÑOS DEL HOGAR Y SE DEBEN CONTAR COMO MIEMBROS DE LA FAMILIA. Para el Niño de Crianza: Sección I Anote a todos los niños en el hogar (asistan o no a la escuela). Anote la escuela del LBUSD o un programa de CDC del LBUSD. Escriba el grado para el año escolar 2015-2016. Marque el casillero en la columna para “Niño de Crianza.” Si todos los niños son niños de crianza, pase a la sección III. Si no todos los niños del hogar son niños de crianza, complete todas las secciones que correspondan y anote el uso personal de ingreso para cada niño de crianza en la Sección II. Firme la solicitud y escriba la fecha Una vez completa, la solicitud se puede entregar a cualquier plantel abierto a cualquier hora durante el dia escolar o a la oficina de Servicios de Nutrición (3333 Airport Way, Long Beach CA 90806). ¿Tiene su niño(a) una dieta especial? Hable con un Especialista en Nutrición Infantil al (562) 427-7923.