transdiagnostic group cbt for anxiety disorder
Anuncio

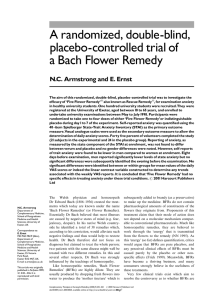
Asociación Española de Psicología Clínica y Psicopatología Revista de Psicopatología y Psicología Clínica Vol. 17, N.º 3, pp. 205-217, 2012 Spanish Journal of Clinical Psychology, www.aepcp.net ISSN 1136-5420/12 TRANSDIAGNOSTIC GROUP CBT FOR ANXIETY DISORDER: EFFICACY, ACCEPTABILITY, AND BEYOND PETER J. NORTON Anxiety Disorder Clinic, Department of Psychology, University of Houston, USA Abstract: Interest in transdiagnostic approaches to the cognitive-behavioral treatment (CBT) of emotional disorders has been increasing over the past decade. The purpose of this paper was to review the rationale behind transdiagnostic treatment models, describe one such group-based treatment protocol in detail, and report on the building evidence base to date. The evidence suggests that transdiagnostic CBT for anxiety is associated with symptom improvement, performs better than waitlist controls, is associated with improvements in comorbid disorders, and performs equivalently to established diagnosis-specific treatments. Transdiagnostic protocols are also associated with good client satisfaction, high levels of therapeutic alliance and group cohesion, and positive treatment perceptions during and following treatment. Limitations and directions for future research are discussed. Keywords: Transdiagnostic; unified; group treatment; emotional disorders, cognitive behavior therapy TCC transdiagnóstica de grupo para los trastornos de ansiedad: Eficacia, aceptabilidad y otros aspectos Resumen: Durante la última década se ha venido incrementando el interés por los enfoques del transdiagnóstico en el tratamiento cognitivo-conductual de los trastornos emocionales. El propósito del presente trabajo consiste en revisar los fundamentos que subyacen a los modelos de tratamiento transdiagnóstico, describir con detalle un protocolo de tratamiento transdiagnóstico de grupo, y proporcionar la evidencia aportada hasta la fecha. La evidencia sugiere que la terapia cognitivo-conductual (TCC) transdiagnóstica de la ansiedad se asocia a mejoría de los síntomas, es superior al grupo de control de lista de espera, y es similar a los tratamientos diagnóstico-específicos ya establecidos. Los protocolos de transdiagnóstico también se han asociado a buena satisfacción del cliente, niveles elevados de alianza terapéutica y cohesión grupal, y percepciones positivas del tratamiento durante el seguimiento. Se discuten las limitaciones y las direcciones para la investigación futura. Palabras clave: Transdiagnóstico; tratamiento unificado; tratamiento de grupo; trastornos emocionales; terapia cognitivo-conductual. 1 Interest in transdiagnostic approaches to the cognitive-behavioral treatment of emotional disorders has been increasing over the past decade, with numerous empirical (e.g., Farchione et al., 2012; Norton, 2012a) and theoretical papers (e.g., Erickson, Janeck, & Tallman, 2009; Norton, 2006), specials issues (see Mansell, 2008; Taylor & Clark, 2009), book chapters Correspondence: Peter J. Norton, Ph.D., Department of Psychology, 126 Heyne Bldg., University of Houston, Houston, TX, 77204-5022, USA, Phone: 713-743-8675, Fax: 713-743-8633. E-mail: [email protected]. 22784_Psicopatologia_17(3)_Cs6.indd 205 (e.g., Fairholme, Boisseau, Ellard, Ehrenreich, & Barlow, 2010; Norton, 2009), and books (e.g., Barlow, Farchione, et al., 2011; Norton, 2012b) being devoted to the topic. At their heart, transdiagnostic approaches to CBT hold that finer clinical distinctions among classes of mental disorders, such as the diagnoses subsumed under the classification of Anxiety Disorders or the specific Eating Disorder diagnoses, are of lesser clinical importance than the broader across-diagnosis (or transdiagnostic) factors inherent to all mental disorders within the larger classification (Harvey, Watkins, Mansell, 10/12/12 09:07 206 Peter J. Norton & Shafran, 2004; Norton, 2006). Indeed, as has been argued elsewhere (Norton, 2006), the expansion of Anxiety Disorder diagnoses from three in DSM-I (American Psychiatric Association [APA], 1952) and DSM-II (APA, 1965) to 25 (including subtypes and specifiers) in DSMIV-TR (APA, 2000), has not yielded substantially unique treatments designed to target the specific features of these diagnoses. Rather, cognitive-behavioral psychotherapies incorporating exposure and cognitive techniques, as well as pharmacological agents impacting the serotonergic system, appear to be similarly efficacious across the Anxiety Disorders when administered in similar doses, regardless of specific diagnosis (Norton & Price, 2007; Hofmann & Smits, 2008; AccessPharmacy, accessed 08/10/2011). As a result, and in response to constraints imposed in attempting to train and deliver multiple CBT treatment programs for specific diagnoses, several investigators (Barlow, Farchione, et al., 2011; Erickson, Janeck, & Tallman, 2007; Norton, 2012b; Schmidt, Buckner, Pusser, Woolaway-Bickel, & Preston, 2012) have developed transdiagnostic CBT programs in order to minimize training demands and maximize treatment accessibility for individuals with anxiety disorders. The current paper will discuss in detail the development and evaluation of one of the most thoroughly studied transdiagnostic treatments for anxiety disorders. TRANSDIAGNOSTIC GROUP CBT FOR ANXIETY DISORDER: DESCRIPTION OF THE PROGRAM In 2002, Norton and Hope (unpublished draft; now published as Norton, 2012b) began developing a transdiagnostic group CBT program in response to two emerging factors. First, considerable data had been mounting from genetic (Andrews, 1991; Andrews, Stewart, Allen, & Henderson, 1990; Andrews, Stewart, MorrisYates, Holt, & Henderson, 1990; Jang, 2005; Jardin, Martin, & Henderson, 1984; Kendler, Heath, Martin, & Eaves, 1987; Kendler, Neale, Kessler, Heath, & Eaves, 1992), personality (Clark & Watson, 1991; Eysenck, 1957; Gray, Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 206 1982; Spielberger, 1985), developmental (Bowlby, 1980; Chorpita & Barlow, 1998; Chorpita, Brown, & Barlow, 1998; Rosenbaum, 2000; Thompson, 2001), psychopathological (Andrews, Stewart, et al., 1990; Brown & Barlow, 1992; Sanderson, Di Nardo, Rapee, & Barlow, 1990), and interventional research (Norton & Price, 2007; Hofmann & Smits, 2008) suggesting that the commonalities across the anxiety disorder diagnoses outweighed the differences (see Norton, 2009). That is, an individual with social anxiety disorder, an individual with agoraphobia, and an individual with a specific phobia of heights, only differ in the specific phenomenon that elicits their fear and anxiety, while the common factors underlying and maintaining the fears are the same. Second, they found that their ability to provide timely clinical services was impaired by an unusual conundrum: patient flow was too high to provide immediate individual CBT to all clients with an anxiety disorder who requested treatment, but patient flow with any specific anxiety disorder diagnosis was too slow to provide timely group CBT for those diagnoses. Indeed, as noted by Norton and Hope (2008), «assuming that all new intakes had an anxiety disorder, it would still require (based on National Comorbidity Survey prevalence estimates) an average 21 intakes before one would expect to have recruited 6 individuals with a primary diagnosis of specific phobia to form the group. It would require 25 intakes for a sixperson social phobia group, 31 intakes for a panic/agoraphobia group, 50 intakes for a PTSD group, 53 intakes for a GAD group, and 199 intakes for an OCD group» (p. 14). In contrast, a transdiagnostic group CBT approach would allow for groups to begin as soon as a sufficient number of patients with any anxiety disorder (e.g., 2 patients with panic disorder, 2 with social anxiety disorder, 2 with generalized anxiety disorder, 1 with OCD, and 1 with PTSD). The transdiagnostic group CBT program (Norton, 2012b; for a group case study, see Norton & Hope, 2008) consists of 12 weekly 2-hour group sessions incorporating six to eight individuals with any anxiety disorder diagnosis. Groups are typically led by two therapists, although they have been success- © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 207 Transdiagnostic CBT for anxiety disorder fully implemented by one experienced therapist on several occasions, and emphasize an overarching philosophy that clients have an excessive or irrational fear of a particular thing (e.g., heights, negative evaluation) as opposed to having diagnoses of panic disorder, OCD, etc. In this way, all clients are seen as sharing the same basic pathology, even though the specific stimuli that trigger the anxiety and the behavioral responses to reduce danger or threat may differ. The group treatment incorporates psychoeducation into the development and maintenance of anxiety, cognitive restructuring of excessive or irrational thoughts underlying the anxiety disorder, graduated exposure and response prevention, cognitive restructuring of core beliefs underlying anxiety, and termination and relapse prevention skills (see Table 1). Table 1. Session-by-session overview of the Transdiagnostic Group CBT program. Session 1 2 Session Content Assigned Homework 10 Psychoeducation and group socialization Psychoeducation and introduction of cognitive restructuring Cognitive restructuring Graduated in-session exposure and response prevention Graduated in-session exposure and response prevention Graduated in-session exposure and response prevention Graduated in-session exposure and response prevention Graduated in-session exposure and response prevention Graduated in-session exposure and response prevention Cognitive restructuring of core beliefs 11 Cognitive restructuring of core beliefs 12 Termination and relapse prevention 3 4 5 6 7 8 9 Prior to Session 1 Before initiating treatment, patients are asked to develop a Fear Hierarchy with a therapist to help guide the treatment. The Fear Hierarchy is a simple list of up to ten situations or stimuli that provoke their anxiety. Hierarchies should ideally comprise a range of situations and stimuli ideographic to that individual, and should address not only situations or stimuli associated with the principal diagnoses but also situations or stimuli associated with © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 207 Self-monitoring of anxiety (ongoing) Monitoring of anxious thoughts Challenging anxious thoughts (ongoing) Self-directed exposure and response prevention Self-directed exposure and response prevention Self-directed exposure and response prevention Self-directed exposure and response prevention Self-directed exposure and response prevention Self-directed exposure and response prevention Monitoring negative-mood inducing core beliefs Challenging negative mood-inducing core beliefs Implementing post-treatment self-therapy plan (ongoing) comorbid anxiety diagnoses. For example, if an individual presented with a principal diagnosis of social phobia and a comorbid diagnosis of OCD, his or her hierarchy might consist of items addressing public speaking and assertiveness (social phobia) as well as contamination and washing (OCD). If possible, variations that make each situation or stimuli more or less anxiety provoking, such as going to a crowded versus relatively deserted mall, should be included. Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07 208 Peter J. Norton Session 1 The first session, which is typically more didactic in structure than the subsequent sessions, is designed to socialize clients to the group format and allow clients to feel more comfortable sharing their personal difficulties. Issues such as attendance, homework completion, confidentiality, and respecting the group members and process (e.g., allowing everyone to contribute) are emphasized. Much of the rest of the session focuses on providing education about the nature of anxiety and anxiety disorder; the cognitive, behavioral, and physiological components of anxiety. An emphasis is placed on normalizing the experience of anxiety, in that anxiety disorders are not a «malfunctioning» of the anxiety and fear systems, but rather their inappropriate activation to stimuli that are either not dangerous or much less dangerous than the individual feels. The three components of anxiety-physiological activation, cognitive shifts toward evidence of danger or threat, and behavioral escape/avoidance motivations-are described to assist the clients in becoming impartial observers of their own anxiety (see Figure 1). Clients are encouraged to describe their own experiences of anxiety, including the triggers that provoke their fears, in an effort to highlight the commonalities and differences in the group’s experience of anxiety and to promote group cohesion. Finally, therapists briefly describe the components of treatment: Education/Self-Monitoring, Specific Cognitive Restructuring, Graduated Exposure, and Generalized Cognitive Restructuring, emphasizing that each component of treatment will require work both in session and at home. Daily self-monitoring of anxiety levels and monitoring the three components of anxiety during a specific anxiety-provoking episode are assigned as homework. Daily self-monitoring is assigned to (a) provide ongoing evaluation of progress throughout treatment, (b) potentially identify previously unknown variables that may exacerbate or mitigate each client’s anxiety, and (c) help the clients become an observer, rather than just an experiencer, of their anxiety. Monitoring the three components during an episode of anxiety is assigned to provide specific client examples Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 208 to be utilized during the introduction to cognitive restructuring in the second session. Cognitive Attention shift to perceived dangers Activation of threatrelevant memories Physiological Increased heart rate, muscle tension, respiration, sweating, etc. Behavioral Motivation to escape or avoid the perceived threat, behavioral rituals to minimize danger Figure 1. Model of the interaction between cognitions, behaviors, and physiological responses. Session 2 The second session focuses primarily on the cognitive component of anxiety. A model is presented that highlights the fact that it is not the stimulus that provokes anxiety, but rather the individual’s interpretation of the stimulus as dangerous or threatening. An example of a household smoke detector is often a good analogy. Should a smoke detector sound its alarm when, for example, someone is cooking bacon, the smoke detector is functioning properly but simply alerting the homeowner of danger when the actual threat is low. This idea is used to introduce the concept of automatic thoughts— over-exaggerated or irrational thoughts of danger or threat that seem to arise automatically when encountering or anticipating the stimuli or situation that a client fears. An example of a hypothetical client is typically provided (e.g., a client with health anxiety concerns that a headache is a sign of a potential stroke) to help clients understand that although the threat feels likely to the individual, there are many more likely interpretations (e.g., the headache could be due to stress, poor sleep, a hangover, etc.). © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 Transdiagnostic CBT for anxiety disorder Clients are then encouraged to identify their own automatic thoughts from commonly occurring situations where they experience anxiety; Probes such as «what did you worry might happen if…,» «what might have happened…,» or «what is the worst that could have happened» may be necessary to elicit automatic thoughts until clients become comfortable with the process of identifying automatic thoughts. As some clients have difficulty in identifying their own automatic thoughts, clients are given strategies for identifying these thoughts in anxiety-provoking situations, such as asking oneself «what am I worried will happen?» whenever they experience a sudden increase in their anxiety or fear. For homework, clients are asked to monitor and record automatic thoughts throughout the week to provide specific individualized examples that can be discussed and challenged during the third session. Clients are also encouraged to continue the daily self-monitoring of their anxiety. Session 3 The third session continues with cognitive strategies in preparation for subsequent sessions that focus on graduated exposure. Automatic thoughts from the previous session homework are reviewed, and the concept of thinking errors is introduced. In this program, Over-Estimation of Probabilities and Catastrophizing the Consequences are specifically highlighted, as they capture the majority of the common misappraisals. Over-estimation of probabilities involves predicting that a feared outcome is likely to occur despite the actual probability being quite low, such as assuming that it is likely one’s airplane will crash. Catastrophizing the consequences, in contrast, involves assuming the worst possible negative feared outcome for something that typically has a more benign consequence, such as fearing that doing something embarrassing will lead to complete rejection and being alone forever. In the group, clients are asked to examine their automatic thoughts to identify thinking errors, which allows other group members to offer input to those clients who may have more © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 209 209 fixed assumptions (e.g., mistaken beliefs in the dangerousness of spiders). Finally, disputing questions designed to assess the actual degree of threat or danger are posed and practiced. Examples of commonly used disputing questions include What evidence do I have that ______ is true/What evidence do I have that ______ is not true? (e.g., What evidence do I have that people are laughing at me/What evidence do I have that people are not laughing at me?) and If ____________ did happen, how bad would it be? (e.g., If I did vomit, how bad would it be?). For homework between sessions, clients are asked to practice and record a full trial of cognitive restructuring of at least one anxiety-producing situation, from identification of automatic thoughts, through identification of thinking errors, to challenging the logic of the automatic thought. Sessions 4 to 9 Sessions 4 through 9 focus on graduated exposure based on each patient’s Fear Hierarchy. Each week, clients will undertake an insession exposure of increasing difficulty, whether in vivo (e.g., touching a surface believed to be contaminated), through simulation (e.g., roleplaying a social interaction), or imaginally (e.g., e.g., cognitive exposure to trauma memories). Prior to each exposure, clients are instructed to use their cognitive restructuring skills to prepare for the exposure. Immediately prior to the beginning of an exposure, the client and therapist should negotiate one or more attainable but challenging behavioral goals that the client should attempt to achieve during the exposure. During all exposures, behavioral strategies designed to reduce anxiety, such as avoidance or compulsive rituals, are identified and prevented during the exposure. During each exposure, the therapists periodically probe for the client’s current level of anxiety (e.g., on a 0-100 scale) to assess the degree to which the exposure is activating the client’s fears and the extent to which the client is habituating during the exposure. The exposure should continue as long as is necessary for the SUDS ratings to climax and begin declining. Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07 210 Peter J. Norton During the first few exposure sessions, most exposures are done individually and sequentially to ensure that they are completed successfully; that is, the therapists will do an exposure with Client A, followed by an exposure with Client B, and so forth. However, in later exposure sessions, exposures among group members may be combined. As noted in Norton (2012b): For example, in a past group we have paired up two clients who both had public speaking fears and had them engage in a formal debate over an innocuous topic. In another group, the clients themselves creatively designed an exposure wherein four clients were able to confront their fears simultaneously. The group left the clinic and walked to a nearby office tower that had a busy cafeteria in it. One socially anxious client made a point to ask multiple strangers in the building for directions to the cafeteria. Another client with claustrophobic fears rode the office elevator up and down multiple floors by herself while a third client, who had concerns that people would be watching her, sat by herself for 10 minutes at a table in the middle of the cafeteria. Finally, a fourth client who had contamination fears touched four surfaces in the cafeteria that he felt might not be clean and refrained from washing his hands. (Norton, 2012b; p. 153) At the conclusion of each exposure session, patients are assigned homework exposures based on the in-session exposure to practice multiple times between sessions in an effort to promote generalization. (Over-Estimation of Probabilities and Catastrophizing the Consequences) and challenged using disputing questions. Although the process is similar to that used on specific automatic thoughts in session 3, core beliefs are typically more firmly entrenched and will usually require a longer period of self-challenging before substantial shifts are observed. Cognitive restructuring homework is assigned following both sessions. Session 12 Finally, during the twelfth session, treatment skills and progress are reviewed, and plans for termination and post-treatment maintenance of gains are developed. Clients are encouraged to reflect on the gains they have made throughout the treatment, and to consider anxiety-relevant ways they can reward themselves. For example, one former group member who overcame substantial agoraphobia rewarded herself by booking a vacation flight—she had not been on an airplane for years due to her fears—to visit family members who lived in another state. Strategies for dealing with stressors and lapses are developed and practiced, and plans for addressing possible return of fears are developed. Finally, plans for continued self-therapy are developed, such as incorporating self-exposure into one’s ongoing lifestyle. Sessions 10 and 11 TREATMENT EFFICACY ON PRINCIPAL ANXIETY DISORDER DIAGNOSES During the tenth and eleventh sessions, the emphasis shift back to cognitions, but with a focus on broader beliefs and schemas underlying the specific fears. Examples of common beliefs or schema have included a belief that anything short of perfection is a failure, a belief that one must always please others to be loved, or a belief that one does not have the skills to cope in a dangerous world. Cognitive restructuring skills akin to those developed in sessions 2 and 3 are employed to begin to soften these broadly held beliefs. Beliefs are examined for any evidence of thinking errors This transdiagnostic group CBT program has been subjected to a considerable amount of empirical research. To begin the empirical evaluation of transdiagnostic group CBT, Norton and Hope (2005) conducted a randomized clinical trial with 23 participants assigned to either transdiagnostic CBT or a waitlist control condition during which the participants did not receive treatment until after the first treatment groups had finished. All participants met DSMIV criteria for a principal anxiety disorder diagnosis, and the following inclusion criteria were established: (1) Age 19 or older, (2) Abil- Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 210 © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 Transdiagnostic CBT for anxiety disorder ity to read and communicate in English, (3) Willingness to accept possibility of randomization to delayed-treatment condition, (4) No evidence of dementia or neurocognitive conditions, and (5) No evidence of suicidality, significant substance abuse, or other condition requiring immediate intervention. Comorbid diagnoses of any kind were acceptable as long as the principal diagnosis was an anxiety disorder. Post-treatment results showed that outcomes on clinician-rated severity (M PRE = 5.44, M POST = 3.04 on a 0-8 scale versus M PRE = 6.45, M POST = 6.07 for waitlist controls), proportion of remitted anxiety disorder diagnoses (67% versus 0% among waitlist controls), and idiographic fear-avoidance hierarchies (M PRE = 70.49, M POST = 37.71 on a 0-100 scale versus M PRE = 67.46, M POST = 62.68 for waitlist controls) were superior for patients receiving treatment as compared to waitlist controls. In a follow-up to the initial study, Norton (2008) conducted an open clinical trial with 52 participants with a principal anxiety disorder diagnosis. Inclusion criteria were identical to the previous (Norton & Hope, 2005) study, with the exception that all participants received immediate transdiagnostic group CBT. Using mixed-effect regression modeling of sessionby-session anxiety severity assessments, Norton (2008) found significant average decreases over the course of treatment such that participants tended to fall outside of the clinical severity range by the end of treatment (M Session 1 = 48.01, M POST = 34.92 on a 20-80 clinical scale). Notably, the results also found no interaction of the treatment effects with diagnosis indicating no differences in improvement for participants with differing anxiety disorder diagnoses (e.g., panic disorder, OCD, etc.). COMPARATIVE TREATMENT EFFICACY WITH ESTABLISHED ANXIETY DISORDER TREATMENTS Given the establishment that transdiagnostic group CBT was associated with significant anxiety reduction, and that no diagnoses were associated with differential improvement, two © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 211 211 comparative outcome trials were undertaken. In the first (Norton, 2012a), 87 participants with an anxiety disorder diagnosis were recruited and randomized to either transdiagnostic group CBT or a group applied relaxation training intervention. Again, inclusion criteria were liberally set to maximize external validity: (1) age 18 or older, (2) ability to read and communicate in English, (3) willingness to accept possibility of randomization to transdiagnostic group CBT or group applied relaxation training, (4) no evidence of dementia or neurocognitive conditions, and (5) no evidence of suicidality, significant substance abuse, or other condition requiring immediate intervention. Analysis of the treatment data using treatment non-inferiority/equivalence methodology suggested equivalent improvement across those receiving transdiagnostic group CBT and those receiving group applied relaxation training, with between group effect sizes all less than η2 = .029. Further, and consistent with the results of Norton (2008), no effects of primary anxiety disorder diagnosis were observed, suggesting that individuals with differing specific anxiety diagnoses showed similar improvement. Subsequently, Norton and Barrera (2012) conducted a randomized controlled trial comparing the efficacy of transdiagnostic group CBT in contrast to diagnosis-specific group CBT, including the Craske and Barlow (2007) Mastery of your Anxiety and Panic (4th ed.) protocol for panic disorder, the Heimberg and Becker (20002) Cognitive-Behavioral Group Therapy for Social Phobia protocol for social anxiety disorder, and the Dugas and Robichaud (2007) Cognitive-Behavioral Treatment for Generalized Anxiety Disorder protocol for GAD. Forty-six individuals with a principal diagnosis of panic disorder, social anxiety disorder, or generalized anxiety disorder who met the same inclusion criteria as the previous trial were randomly assigned to transdiagnostic or diagnosis-specific group CBT. Analyses were again conducted using a treatment equivalence/ non-inferiority methodology, and largely found equivalence in outcomes between the transdiagnostic and diagnosis-specific CBT formats, with between groups effect sizes all less than η2 = .052. Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07 212 Peter J. Norton EFFECT OF TRANSDIAGNOSTIC GROUP CBT ON COMORBID DIAGNOSES Traditional CBT delivered for specific diagnoses has repeatedly shown indirect effects on comorbid anxiety and depressive diagnoses (e.g., Allen et al., 2010; Brown, Antony, & Barlow, 1995; Tsao et al., 1998, 2002, 2005), although such effects have been fairly modest with only approximately 41.4% of individuals with comorbid emotional diagnoses showing remittance of these comorbid diagnoses at posttreatment (21.4% to 57.1%; see Norton, Barrera, Mathew, Chamberlain, Szafranski, et al., in press). However, Mansell, Harvey, Watkins, and Shafran (2009), McEvoy, Nathan, and Norton (2009), and McManus, Shafran, and Cooper (2010) have all proposed that transdiagnostic CBT may hold an advantage over diagnosisspecific CBT in reducing comorbidity, as the patients’ entire anxiety presentation is targeted as opposed to only the features of one diagnosis. To test this, Norton, Hayes, and Hope (2004) conducted a secondary analysis of the Norton and Hope (2005) data and found significant decreases in depressed mood for clients undergoing transdiagnostic treatment for anxiety when compared to waitlist control participants. Seventy-five percent of participants with a comorbid depressive disorder receiving transdiagnostic group CBT showed remittance of their depressive diagnoses to subclinical levels, whereas no change in depressive severity occurred for those in the waitlist control condition. Similarly, substantial improvement on selfreport indices of depressive severity was observed for those receiving immediate treatment whereas no change was observed for waitlist controls. Similarly, Norton et al (in press) reanalyzed data from participants assigned to the transdiagnostic group CBT condition in the Norton (2008), Norton (2012a), and Norton and Barrera (2012) clinical trials. Consistent with diagnosis-specific treatment trials, a majority of clients (64.6%) had at least one comorbid disorder, and a substantially higher percentage (66.7%) of participants receiving transdiagnostic group CBT showed full remittance of all comorbid diagnoses than is typical with diag- Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 212 nosis-specific CBT (48.5%). Similarly superior effects on comorbid diagnoses have also been reported following completion of other transdiagnostic CBT programs (see Ellard et al., 2010). PROCESS OF CHANGE IN TRANSDIAGNOSTIC GROUP CBT Given the strong efficacy data, both on primary outcomes as well as comorbid diagnoses, research on transdiagnostic group CBT has increasingly begun to examine the processes and mechanisms underlying the treatment and its outcomes. Norton, Klenck, and Barrera (2010), for example, examined the trajectories of improvement throughout the course of the 12-week transdiagnostic group CBT. Although the majority of participants evidenced steady incremental improvement across sessions, roughly one-fifth of clients experienced at least one sudden gain, defined as a large and relatively stable decrease in symptoms between subsequent sessions. These participants who experienced a sudden gain showed greater overall improvement following treatment than did clients who did not experience a sudden gain. Interestingly, those who experienced a sudden gain showed greater cognitive shifts (i.e., greater awareness of the irrationality of their anxious thoughts or greater acceptance of alternative non-anxious interpretations) in the pregain session than did those not showing a sudden gain. Norton, Hayes, and Springer (2008) questioned the extent to which the transdiagnostic approach impacted upon therapeutic processes, such as group cohesion, treatment credibility, or therapeutic alliance. They examined treatment process variables from a sample of 54 individuals with an anxiety disorder diagnosis who participated in the Norton (2008) clinical trial. Results suggested strong and increasing therapist therapeutic alliance and group cohesion throughout treatment at levels similar to those seen in trials of diagnosisspecific CBT. Furthermore, stronger alliance and cohesion were generally related to better outcomes. © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 Transdiagnostic CBT for anxiety disorder Chamberlain and Norton (in press) examined the extent to which the diagnostic composition of the CBT groups might impact the cohesiveness of the group as well as the efficacy of the treatment, as it is possible that patients in more diagnostically homogeneous groups may identify more closely with each other. Individual indices of diagnostic composition based upon the number of group members sharing similar anxiety disorder diagnoses were employed to explore potential differences in treatment outcome related to the diagnostic makeup of the treatment group. Results indicated that the diagnostic makeup of the treatment group had little, if any, impact on individual treatment outcome, suggesting that transdiagnostic CBT groups can be formed efficiently without concern for the specific anxiety disorder diagnoses of those being enrolled in each group. Finally, Smith, Norton, and McLean (in press) conducted an analysis of data from participants in the Norton (2008), Norton (2012a), and Norton and Barrera (2012) studies to examine patient perceptions of the aspects of therapy that they felt were most beneficial. Although all aspects of treatment were favorably rated by the patients, treatment response was significantly correlated with perceived helpfulness of cognitive restructuring and exposures, but not other treatment factors, suggesting that those patients who improved the most identified the active ingredients of CBT as the most beneficial. Indeed, the importance of graduated exposure and response prevention in transdiagnostic group CBT was highlighted by Norton, Hayes, and Klenck (2011). They analyzed the impact of activation and habituation during within-session exposures on subsequent between-session anxiety reduction among clients with a range of anxiety disorders. Results revealed patients who experienced a poorer first exposure (i.e., clients not habituating or increasing in anxiety) were significantly more likely to subsequently discontinue treatment, while those experiencing successful later exposures where larger increases and decreases in anxiety during the exposure (i.e., activation and habituation) were generally associated with better treatment outcomes. © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 213 213 OTHER TRANSDIAGNOSTIC CBT PROGRAMS FOR ANXIETY In addition to the works described above, several other psychological research teams have independently developed similar transdiagnostic CBT programs for the treatment of anxiety and emotional disorders, although the extent of the evidence base supporting the efficacy of these treatments varies considerably (see Norton & Philipp, 2008 for a quantitative review). The most extensively investigated of these alternative transdiagnostic CBT programs is that of Barlow, Farchione, Fairholme, Ellard, Boisseau, et al. (2011), called the Unified Protocol (UP). UP is an emotion-focused individual CBT for the broad range of anxiety and mood disorders, although the majority of the research into the efficacy of UP has focused on individuals with anxiety disorder diagnoses (Ellard et al., 2010). Prior to beginning UP, a brief Motivational Interviewing module is delivered, followed by five modules to be delivered over a maximum of 18 one-hour sessions: Increasing present-focused emotional awareness; Facilitating flexibility in cognitive appraisals; Identifying and preventing maladaptive behavioral and emotional avoidance; Increasing tolerance of emotion-related physiological sensations; and Interoceptive and situational exposures to emotional cues. Termination and relapse prevention skills are provided at the completion of the UP protocol. Ellard et al. (2010) reported significant improvement on anxiety and functioning during two open trials of UP, particularly after modifying the protocol in response to the first trial. Farchione et al. (2012) reported on a randomized clinical trial of UP in comparison to a waitlist control condition, finding that those receiving UP showed significant improvement on indices of anxiety severity, depressive symptoms, and negative and positive affectivity. The Unified Protocol therapist manual (Barlow, Farchione, et al., 2011) and client workbook (Barlow, Ellard, et al., 2011) are available for purchase. McEvoy and Nathan (2007) reported data from a trial of a transdiagnostic group CBT protocol for anxiety and affective disorders. The group treatment program, which typically in- Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07 214 Peter J. Norton cludes 8 to 10 patients, occurs over 10 weekly 2-hour sessions followed by an individual booster session one month later. The protocol covers psychoeducation about anxiety and depression, behavioral activation and graded exposure, calming techniques, and cognitive restructuring skills. Each session also included weekly goal setting and review of homework, as well as an emphasis on the regular use of calming techniques. McEvoy and Nathan found that patients in their transdiagnostic group CBT program showed a similar degree of improvement to what was seen in studies of diagnosisspecific CBT. The protocol (Nathan, Rees, & Smith, 2001) is available for purchase through the authors. Schmidt and colleagues (2012) recently reported efficacy data for a transdiagnostic group CBT program entitled False Safety Behavior Elimination Therapy (F-SET; Schmidt & Woolaway-Bickel, 2002) for individuals diagnosed with panic disorder, social anxiety disorder, or generalized anxiety disorder. F-SET is comprised of 10 weekly 2-hour group sessions. During the initial sessions, clients are educated about the importance of thoughts and behaviors in anxiety disorders, with a specific focus on what Schmidt and Woolaway-Bickel refer to as False Safety Behaviors—behaviors used to reduce perceptions of danger despite the actual degree of threat being low. During subsequent sessions, false safety behaviors are reduced or eliminated while clients are encouraged to engage in activities that are opposite to their anxious tendencies. The results of the Schmidt et al. (2012) clinical trial found that, compared to participants randomly assigned to a waitlist control condition, participants receiving F-SET showed significant improvements across of range of indices of anxiety severity, when delivered by relatively inexperienced clinicians. The public availability of the F-SET protocol is currently unknown. Erickson, Janeck, and Tallman (2007) reported data from a randomized clinical trial assessing the efficacy of a transdiagnostic group CBT protocol for Mixed Anxiety Groups (MAG), which was based on a previous transdiagnostic CBT protocol (Erickson, 2003). The initial protocol was developed to be fully trans- Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 214 diagnostic across the anxiety disorders, although Erickson et al. (2009) later suggested restriction to patients with principal diagnoses of panic disorder, social anxiety disorder, generalized anxiety disorder, and specific phobia. The MAG protocol consists of 11 weekly sessions, each lasting 2 hours. Groups are larger than in the other transdiagnostic group CBT programs, consisting of up to 12 clients. During sessions 1 and 2, clients develop a fear hierarchy and practice goal setting, while session 3 involves the introduction of in vivo exposure, cognitive reappraisal, interoceptive exposure, and scheduled worry time. During sessions 4 and 5, and again during session 8, diaphragmatic breathing and progressive muscle relaxation are introduced and practiced, while sessions 6, 7, and 9 involve identifying and challenging automatic thoughts. Finally, during sessions 10 and 11, strategies for relapse prevention are developed and termination issues are discussed. The results of their clinical trial indicated that those receiving transdiagnostic group CBT improved more than participants randomized to delayed treatment waitlist control condition. The public availability of the MAG protocol is currently unknown. CONCLUSIONS AND FUTURE DIRECTIONS Overall, the evidence to date strongly converges in support of the efficacy of transdiagnostic CBT for the treatment of anxiety disorders. All of the trials showed signif icant reductions in the severity of anxiety among those receiving transdiagnostic CBT (e.g., Norton & Hope, 2005), and no evidence that any specific anxiety disorder diagnoses respond less favorably to these treatments (Norton, 2008). Two trials (Norton, 2012 and Norton & Barrera, 2012, respectively) have found that transdiagnostic CBT is equally efficacious as applied relaxation training and traditional diagnosis-specif ic CBT when considering principal diagnoses, and possibly more so through their apparent greater impact on comorbid anxiety and depressive diagnoses (Norton et al., 2004; Norton et al., in press). Interestingly, despite initial concerns over the © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 Transdiagnostic CBT for anxiety disorder feasibility of combining individuals with fears of different stimuli in the same treatment group, several studies (Chamberlain & Norton, in press; Norton, Hayes, & Springer, 2008) have shown no impact of the diagnostically mixed groups on either group cohesion or on outcomes, and patients typically report favorable impressions of the treatment (Norton, Hayes, & Springer, 2008; Smith, Norton, & McLean, in press). Of course, more research needs to be conducted and, in some cases is underway. Most notably, the findings of equivalent outcomes between transdiagnostic and diagnosis-specific CBT need to be replicated in additional samples. Ideally, such trials should be conducted by other independent research teams, as all of the published outcome studies have involved the treatment developers and therefore their data may have been influenced by allegiance effects. Similarly, the data suggesting higher rates of remission for comorbid diagnoses following transdiagnostic CBT than is typically seen in diagnosis-specific CBT (Norton et al., in press) needs to be directly evaluated in a comparative outcome trial. Finally, representation of individuals with principal diagnoses of obsessive-compulsive disorder and post-traumatic stress disorder in these trials has been limited, either by design (Schmidt et al., 2012) or as a consequence of patient flow (Norton, 2008); therefore future trials are necessary to establish the appropriateness of transdiagnostic CBT among individuals with these diagnoses. Finally, the effectiveness, acceptability, and feasibility of transdiagnostic CBT when implemented in general clinical practice in the community has not been systematically evaluated, and remains a key area for future research. Even so, the research conducted and published to date show excellent promise for transdiagnostic approaches to CBT for anxiety disorders. REFERENCES AccessPharmacy (accessed 08/10/2011). Pharmacotherapy: A Pathophysiologic Approach, 8e > Section 7. Psychiatric Disorders > Chapter 79. Anxiety Disorders © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 215 215 I: Generalized Anxiety, Panic, and Social Anxiety Disorders. McGraw/Hill. AccessPharmacy (accessed 08/10/2011). Pharmacotherapy: A Pathophysiologic Approach, 8e > Section 7. Psychiatric Disorders > Chapter 80. Anxiety Disorders II: Posttraumatic Stress Disorder and Obsessive-Compulsive Disorder. McGraw/Hill. Allen, L. B., White, K. S., Barlow, D. H., Shear, K. M., Gorman, J. M., & Woods, S. W (2010). Cognitive-behavior therapy (CBT) for panic disorder: Relationship of anxiety and depression comorbidity with treatment outcome. Journal of Psychopathology and Behavioral Assessment, 32, 185-192. American Psychiatric Association (2000). Diagnostic and statistical manual for mental disorders (4th ed., text rev.). Washington, DC: Author. American Psychiatric Association. (1965). Diagnostic and statistical manual of mental disorders (2nd ed.). Washington, D.C.: Author. American Psychiatric Association. (1952). Diagnostic and statistical manual of mental disorders. Washington, D.C.: Author. Andrews, G. (1991). Anxiety, personality, and anxiety disorders. International Review of Psychiatry, 3, 293-302. Andrews, G., Stewart, G. W., Allen, R., & Henderson, A. S. (1990). The genetics of six neurotic disorders: A twin study. Journal of Affective Disorders, 19, 23-29. Andrews, G., Stewart, G. W., Morris-Yates, A., Holt, P. E., & Henderson, A. S. (1990). Evidence for a general neurotic syndrome. British Journal of Psychiatry, 157, 6-12. Barlow, D.H., Ellard, K.K., Fairholme, C.P., Farchione, T.J., Boisseau, C.L. Allen, L.B. & Ehrenreich-May, J. (2011). The unified protocol for transdiagnostic treatment of emotional disorders: Client workbook. New York, NY: Oxford University Press. Barlow, D. H., Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau, C. L. Allen, L. B. & Ehrenreich-May, J. (2011). The unified protocol for transdiagnostic treatment of emotional disorders: Therapist guide. New York, NY: Oxford University Press. Bowlby, J. (1980). Attachment and loss: Vol. 3. Loss, sadness, and depression. New York: Basic Books. Brown, T. A., Antony, M. M., & Barlow, D. H. (1995). Diagnostic comorbidity in panic disorder: Effect on treatment outcome and course of comorbid diagnoses following treatment. Journal of Consulting and Clinical Psychology, 63, 408-418. Brown, T. A. & Barlow, D. H. (1992). Comorbidity among anxiety disorders: Implications for treatment and DSMIV. Journal of Consulting and Clinical Psychology, 60, 835-844. Chamberlain, L. D. & Norton, P. J. (in press). The impact of diagnostic heterogeneity on outcomes in transdiagnostic group CBT for anxiety. Cognitive Behaviour Therapy. Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07 216 Peter J. Norton Chorpita, B. F. & Barlow, D. H. (1998). The development of anxiety: The role of control in the early environment. Psychological Bulletin, 124, 3-21. Chorpita, B. F., Brown, T. A., & Barlow, D. H. (1998). Perceived control as a mediator of family environment in etiological models of childhood anxiety. Behavior Therapy, 29, 457-476. Clark, L. A. & Watson, D. (1991). Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. Journal of Abnormal Psychology, 100, 316-336. Craske, M. G. & Barlow, D. H. (2007). Mastery of your anxiety and panic (4th ed.). New York, Oxford; 2007. Dugas, M. J. & Robichaud, M. (2007). Cognitive-behavioral treatment for generalized anxiety disorder: From science to practice. New York: Routledge. Ellard, K. K., Fairholme, C. P., Boisseaux, C. L., Farchione, T. J., & Barlow, D. H. (2010). Unified protocol for the transdiagnostic treatment of emotional disorders: Protocol development and initial outcome data. Cognitive and Behavioral Practice, 17, 88-101. Erickson, D. H. (2003). Group cognitive behavioural therapy for heterogeneous anxiety disorders. Cognitive Behaviour Therapy, 32, 179-186. Erickson, D. H., Janeck, A., & Tallman, K. (2009). Transdiagnostic group CBT for anxiety: Clinical experience and practical advice. Journal of Cognitive Psychotherapy, 23, 34-43. Erickson, D. H., Janeck, A. S., & Tallman, K. (2007). A cognitive-behavioral group for patients with various anxiety disorders. Psychiatric Services, 58, 1205-1211. Eysenck, H. J. (1957). The dynamics of anxiety and hysteria: An experimental application of modern learning theory to psychiatry. London: Routledge & Kegan Paul. Fairholme, C. P., Boisseau, C. L., Ellard, K. K., Ehrenreich, J. T., & Barlow, D. H. (2010). Emotions, emotion regulation, and psychological treatment: A unified perspective. In A. M. Kring & D. M. Sloan (Eds.), Emotion regulation and psychopathology: A transdiagnostic approach to etiology and treatment. (pp. 283-309). New York, NY US: Guilford Press. Farchione, T. J., Fairholme, C. P., Ellard, K. K., Boisseau, C. L., Thompson-Hollands, J., Carl, J. R., Gallagher, M. & Barlow, D. H. (2012).The unified protocol for the transdiagnostic treatment of emotional disorders: A randomized controlled trial. Behavior Therapy, 43, 666-678. Gray, J. A. (1982). The neurobiology of anxiety. New York: Oxford University Press. Harvey, A.G., Watkings, E., Mansell, W. & Shafran, R. (2004), Cognitive behavioural processes across psychological disorders: A transdiagnostic approach to research and treatment. Oxford University Press. Heimberg, R. G. & Becker, R. E. (2002). Cognitive-behavioral group therapy for social phobia: Basic mech- Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 22784_Psicopatologia_17(3)_Cs6.indd 216 anisms and clinical strategies. New York: Guilford Press. Hofmann, S. G. & Smits, J. A. J. (2008). Cognitive-behavioral therapy for adult anxiety disorders: A meta-analysis of randomized placebo-controlled trials. Journal of Clinical Psychiatry, 69, 621-632. Jang, K. L. (2005). The behavioral genetics of psychopathology: A clinical guide. Mahwah, NJ: Erlbaum. Jardin, R., Martin, N. G., & Henderson, A. S. (1984). Genetic covariation between neuroticism, and the symptoms of anxiety and depression. Genetics Epidemiology, 1, 89-107. Kendler, K. S., Heath, A. C., Martin, N. G., & Eaves, L. J. (1986). Symptoms of anxiety and depression in a volunteer twin population. Archives of General Psychiatry, 43, 213-221. Kendler, K. S., Neale, M. C., Kessler, R. C., Heath, A. C., & Eaves, L. J. (1992). Major depression and generalized anxiety disorder: Same genes, (partly) different environments? Archives of General Psychiatry, 49, 716-722. Manning, J. J., Hooke, G. R., Tannenbaum, D. A., Blythe, T. H., & Clarke, T. M. (1994). Intensive cognitivebehaviour group therapy for diagnostically heterogeneous groups of patients with psychiatric disorder. Australian and New Zealand Journal of Psychiatry, 28, 667-674. Mansell, W., Harvey, A., Watkins, E., & Shafran, R. (2009). Conceptual foundations of the transdiagnostic approach to CBT. Journal of Cognitive Psychotherapy: An International Quarterly, 23, 6-19. McEvoy, P. M., & Nathan, P. (2007). Effectiveness of cognitive behaviour therapy for diagnostically heterogenous groups: A benchmarking study. Journal of Consulting and Clinical Psychology, 75, 344-350. McEvoy, P. M., Nathan, P., & Norton, P. J. (2009). Efficacy of transdiagnostic treatments: A review of published outcome studies and future research directions. Journal of Cognitive Psychotherapy, 23, 27-40. McManus, F., Shafran, R., & Cooper, Z. (2010). What does a ‘transdiagnostic’ approach have to offer the treatment of anxiety disorders? British Journal of Clinical Psychology, 49, 491-505. Nathan, P. R., Rees, C. S., & Smith, L. M. (2001). Mood management course: A group cognitive behavioural programme for anxiety disorders and depression. Perth, Australia: Rioby. (Available from http://www.cci. health.wa.gov.au/index.html) Norton, P. J. (2012a). A randomized clinical trial of transdiagnostic CBT for anxiety disorder by comparison to relaxation training. Behavior Therapy, 43, 506-517. Norton, P. J. (2012b). Group cognitive-behavioral therapy of anxiety: A transdiagnostic treatment manual. New York: Guilford. © Asociación Española de Psicología Clínica y Psicopatología 10/12/12 09:07 Transdiagnostic CBT for anxiety disorder Norton, P. J. (2009). Integrated psychological treatment of multiple anxiety disorders. In: M. M. Antony and M. B. Stein (Eds.), Handbook of anxiety and the anxiety disorders. New York: Oxford. Norton, P. J. (2008). An open trial of a transdiagnostic cognitive-behavioral group therapy for anxiety disorder. Behavior Therapy, 39, 242-250. Norton, P. J. (2006). Toward a clinically-oriented model of anxiety disorders. Cognitive Behaviour Therapy, 35, 88-105. Norton, P. J. & Barrera, T. L. (2012). Transdiagnostic versus diagnosis-specific CBT for anxiety disorders: A preliminary randomized controlled trial. Depression and Anxiety, 29, 874-882. Norton, P. J., Barrera, T. L., Mathew, A. R., Chamberlain, L. D., Szafranski, D. D., Reddy, R., & Smith, A. H. (in press). Effect of transdiagnostic CBT for anxiety on comorbid diagnoses. Depression and Anxiety. Norton, P. J., Hayes, S. A., & Hope, D. A. (2004). Effects of a transdiagnostic group treatment for anxiety on secondary depressive disorders. Depression and Anxiety, 20, 198-202. Norton, P. J., Hayes, S. A., & Klenck, S. C. (2011). What happens in session doesn’t stay in session: Changes within exposures predict subsequent improvement and dropout. Journal of Anxiety Disorders, 25, 654-660. Norton, P. J., Hayes, S. A., & Springer, J. R. (2008). Transdiagnostic cognitive-behavioral group therapy for anxiety: Outcome and process. International Journal of Cognitive Therapy, 1, 266-279. Norton, P. J. & Hope, D. A. (2008). The «Anxiety Treatment Protocol»: A Group Case Study Demonstration of a Transdiagnostic Group CBT for Anxiety Disorders. Clinical Case Studies, 7, 538-554. Norton, P. J. & Hope, D. A. (2005). Preliminary evaluation of a broad-spectrum cognitive-behavioral group therapy for anxiety. Journal of Behavior Therapy and Experimental Psychiatry, 36, 79-97. Norton, P. J., Klenck, S. C., & Barrera, T. L. (2010). Sudden changes during cognitive behavioral group therapy for anxiety disorders. Journal of Anxiety Disorders, 24, 887-892. Norton, P. J. & Philipp, L. M. (2008). Transdiagnostic approaches to the treatment of anxiety disorders: A meta-analytic review. Psychotherapy: Theory, Research, Practice, and Training, 45, 214-226. Norton, P. J. & Price, E. P. (2007). A meta-analytic review of cognitive-behavioral treatment outcome across the anxiety disorders. Journal of Nervous and Mental Disease, 195, 521-531. © Asociación Española de Psicología Clínica y Psicopatología 22784_Psicopatologia_17(3)_Cs6.indd 217 217 Rosenbaum, J. F. (March, 2000). Childhood origins of panic disorder. In J. C. Ballenger & M. K. Shear (Chairs), Milestones and the millennium series: Panic disorder. Symposium presented at the 20 annual meeting of the Anxiety Disorders Association of America, Washington, DC. Sanderson, W. C., Di Nardo, P. A., Rapee, R. M., & Barlow, D. H. (1990). Syndrome comorbidity in patients diagnosed with a DSM-III-R anxiety disorder. Journal of Abnormal Psychology, 99, 308-312. Schmidt, N. B., Buckner, J. D. Pusser, A., Woolaway-Bickel, K., & Preston, J. L. (2012). Randomized controlled trial of False Safety Behavior Elimination Therapy (F-SET): A unified cognitive behavioral treatment for anxiety psychopathology. Behavior Therapy, 43, 518-532. Schmidt, N. B., & Woolaway-Bickel, K. (2002). Defeating anxiety: False safety aid treatment (F-SET). Unpublished treatment manual. Smith, A. H., Norton, P. J., & McLean, C. P. (in press). Client perceptions of therapy component helpfulness in group cognitive-behavioral therapy for anxiety disorders. Journal of Clinical Psychology. Speilberger, C. D. (1985). Anxiety, cognition and affect: A state-trait perspective. In A. H. Tuma & J. D. Maser (Eds.), Anxiety and the anxiety disorders (pp. 171-182). Hillsdale, NJ: Lawrence Erlbaum. Taylor, S. & Clark, D. A. (2009). Transdiagnostic cognitive-behavioral treatments for mood and anxiety disorders: Introduction to the special issue. Journal of Cognitive Psychotherapy, 23, 3-5. Thompson, R. A. (2001). Childhood anxiety disorders from the perspective of emotion regulation and attachment. In M. W. Vasey & M. R. Dadds (Eds.), The developmental psychopathology of anxiety (pp. 160-182). New York: Oxford University Press. Tsao, J. C., Lewin, M. R., & Craske, M. G. (1998). The effects of cognitive-behavioral therapy for panic disorder on comorbid conditions. Journal of Anxiety Disorders, 12, 357-371. Tsao, J. C., Mystkowski, J. L., Zucker, B. G., & Craske, M. G. (2002). Effects of cognitive-behavioral therapy for panic disorder on comorbid conditions: Replication and extension. Behavior Therapy, 33, 493-509. Tsao, J. C., Mystkowski, J. L., Zucker, B. G., & Craske, M. G. (2005). Impact of cognitive-behavioral therapy for panic disorder on comorbidity: A controlled investigation. Behaviour Research & Therapy, 43, 959-970. Revista de Psicopatología y Psicología Clínica 2012, Vol. 17 (3), 205-217 10/12/12 09:07