Changing Patterns in HIV Reverse Transcriptase Resistance
Anuncio

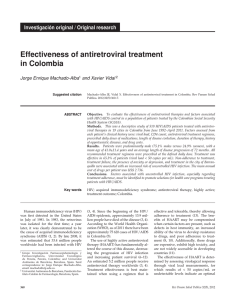
HIV/AIDS BRIEF REPORT Changing Patterns in HIV Reverse Transcriptase Resistance Mutations after Availability of Tenofovir Carmen de Mendoza,1 Inmaculada Jiménez-Nacher,2 Carolina Garrido,1 Pablo Barreiro,1 Eva Poveda,1 Angélica Corral,1 Natalia Zahonero,1 Juan González-Lahoz,1 and Vincent Soriano1 1 Department of Infectious Diseases and 2Pharmacy Unit, Hospital Carlos III, Madrid, Spain Assessment of 1177 human immunodeficiency virus (HIV) resistance genotypes at an HIV/AIDS clinic showed a decrease in the incidence of the K65R mutation, from 15.2% of isolates during the period 2002–2004 to 2.7% of isolates during the period 2005–2006 (P ! .001 ), despite elevated and stable rates of tenofovir use. A reduction in the rate of coadministration of didanosine (from 41.6% of patients in 2004 to 0.8% of patients in 2006; P ! .001) largely explained this observation. Current guidelines recommend the use of tenofovir disoproxil fumarate (TDF) as one of the preferred nucleoside reversetranscriptase inhibitors (NRTI) for first-line antiretroviral therapy [1]. TDF was marketed in Spain in June 2002, although the drug had been widely available within an expanded access program since the middle of 2001. Three main different patterns of drug resistance mutations may confer loss of susceptibility to TDF. K65R is the primary TDF resistance change in drug-naive subjects, and its selection clearly correlates with an impaired response to the drug [2]. In addition, K65R is known to reduce susceptibility to all other NRTIs except zidovudine [2]. Not surprisingly, the rate of K65R rapidly increased after TDF approval [3]. The other resistance mutations compromising TDF activity are T69S inserts and ⭓3 thymidine-associated mutations (TAMs), including M41L and L210W [4, 5]. The emergence of the K70E mutation has also recently been linked to failure of TDF therapy [6]. The aim of Received 9 July 2007; accepted 28 December 2007; electronically published 21 April 2008. Presented in part: 5th European HIV Resistance Workshop, Cascais, Portugal, 28–30 March 2007. Reprints or correspondence: Dr. Carmen de Mendoza, Laboratory of Molecular Biology, Dept. of Infectious Diseases, Hospital Carlos III, Calle Sinesio Delgado 10, 28029 Madrid, Spain ([email protected]). Clinical Infectious Diseases 2008; 46:1782–5 2008 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2008/4611-0023$15.00 DOI: 10.1086/588045 1782 • CID 2008:46 (1 June) • HIV/AIDS this study was to assess retrospectively trends in the prevalence of these TDF-associated resistance patterns and determine which factors are associated with their selection in a relatively large population of patients treated with TDF. Patients and methods. All HIV drug resistance tests performed during the period January 2000–December 2006 on samples from antiretroviral-experienced patients with plasma HIV RNA levels 11000 copies/mL in a reference laboratory located in Madrid, Spain, were retrospectively examined. A case report form was filled out for each sample, in which sex, age, risk category, viral load, CD4+ cell count, and current and past antiretroviral therapies were recorded in a computerized database. HIV pol sequences were generated from plasma specimens. Genetic sequence analyses were performed using ViroSeq (Abbott Molecular Diagnostics). For the purpose of this study, only mutations associated with reduced susceptibility to TDF, according to the latest International AIDS Society–USA panel list, were considered [7]. To compare trends in the emergence of TDF-associated resistance patterns over time with changes in the prescription of antiretroviral therapy, the proportion of patients receiving antiretroviral therapy—and specifically, the number receiving TDF—was recorded using clinical charts and the hospital pharmacy registry. Results. After the approval of TDF in Spain, its use rapidly increased; at the end of 2002, it was prescribed to 400 individuals (40% of all patients receiving HAART in Spain). The number further increased to 745 patients (70% of those receiving HAART) in 2003, with relative stabilization since then: 755 patients (59% of those receiving HAART) in 2004, 719 (54%) in 2005, and 736 (54%) in 2006. Trends in TDF prescription in combination with other NRTIs significantly changed over time. TDF plus didanosine was one of the most widely used combinations during 2002 and 2003 (used in 36% of patients receiving TDF). However, by 2006, the coformulated combination of TDF plus emtricitabine was taken by 180% of patients receiving TDF (figure 1). Of a total of 1177 samples examined, obtained from 767 different patients with HIV infection who were experiencing failure of antiretroviral therapy during the study period and for whom drug resistance testing results were available, 374 (31.7%) were from patients who experienced failure of treatment with TDF. If the study period was restricted to the time since TDF was marketed, 996 samples from patients who experienced failure of antiretroviral therapy were available for analysis; of these, 374 (37.5%) belonged to patients who ex- Figure 1. A, Absolute number of patients receiving HAART, absolute number of patients receiving tenofovir (TDF), and proportion of patients receiving HAART who were treated with TDF. B, frequency of TDF coadministration with nucleoside reverse-transcriptase inhibitors. ABC, abacavir; ddI, didanosine; FTC, emtricitabine; 3TC, lamivudine. perienced failure of treatment with TDF. As expected, virus with TDF-associated resistance mutations was significantly more prevalent among patients who experienced failure of TDF therapy than among patients experiencing failure of treatment with other NRTI-containing regimens (table 1). Of note, all but 1 K70E mutation occurred in isolates from patients with virus harboring either K65R or ⭓3 TAMs. The rate of distinct TDF-associated resistance patterns changed significantly over time. K65R was found in !1% of isolates before 2001; however, the rate of K65R rapidly increased to 14% of isolates in 2002, which was coincident with TDF marketing. It decreased to 2.7% of isolates in the period 2005– 2006 (P ! .001). In contrast, the rate of ⭓3 TAMs steadily increased, from 33% of isolates in the period 2002–2004 to 44.1% of isolates in the period 2005–2006 (P p .02). The prevalence of T69S inserts remained fairly stable at ∼1% over the entire study period (figure 2). Overall, the decrease in the incidence of K65R was mainly associated with a reduction in the prescription of the combination of TDF plus didanosine, which accounted for 41.6% of all TDF-including regimens in 2003 but only 0.8% of such regimens in 2006 (P ! .001). In the univariate analysis, selection of K65R in patients receiving TDF regimens was associated with coadministration of didanosine, compared with administration of another NRTI (20.3% vs. 5.9%; P ! .001) and compared with administration of abacavir (26.2% vs. 8.1%; P ! .001). No statistically significant association was found between selection of K65R and administration of other NRTIs, such as lamivudine or stavudine. Conversely, a significant inverse correlation was observed for K65R in patients who were experiencing failure of TDF therapy and were receiving zidovudine concomitantly, because none of these patients had virus that developed K65R (0% vs. 11.8%; P p .042). In the multivariate analysis, the prescription of TDF, didanosine, abacavir, and M184V were independently associated with the presence of K65R, whereas the number of TAMs was inversely associated with the presence of K65R (table 2). Discussion. TDF is currently one the most widely used NRTIs for the treatment of HIV infection. Its efficacy, favorable toxicity profile, and convenient dosing have made this drug one of—if not the most—popular for first-line treatment, as has been recorded in several guidelines [1]. However, the emergence of drug resistance (and, specifically, selection of K65R) has been a matter of concern in patients who experience failure of TDF therapy, because K65R may result in broad cross-resistance (it currently confers resistance to all NRTIs except zidovudine) [7]. In this study, we assessed the prevalence of TDF-associated resistance mutations in a relatively large group of patients who experienced failure of antiretroviral therapy and trends since the marketing of TDF in Spain in 2002. The overall prevalence of virus with TDF-associated resistance mutations in patients who experienced failure of TDFcontaining regimens was relatively low in this study (!15%), except for the pattern of ⭓3 TAMs including M41L and/or L210W, which had an overall prevalence of 36.6%. Our study shows that selection of K65R is associated with exposure not only to TDF but also to didanosine and abacavir. In other studies, K65R was selected in up to 4% of persons experiencing treatment failure of first-line regimens based on stavudine, lamivudine, and efavirenz [8]. This observation is consistent with the fact that K65R may compromise the antiviral activity of all NRTIs other than TDF (except for zidovudine) [2]. HIV/AIDS • CID 2008:46 (1 June) • 1783 Table 1. Tenofovir (TDF)–associated resistance mutations in the study population. Mutation All patients (n p 1177) K65R T69 inserts K70E ⭓3 TAMs (with M41L or L210W) 50 15 4 350 (4.2) (1.3) (0.3) (29.7) Patients who experienced failure of HAART with TDF (n p 374) 42 8 4 137 (11.2) (2.1) (1.1) (36.6) Patients who experienced failure of HAART without TDF (n p 803) 8 7 0 213 (1) (0.9) (0) (26.5) P .001 .092 .01 .001 NOTE. Data are no. (%) of patients with virus with the specified mutation. TAM, thymidine-associated mutation. We and others have previously reported that the rate of K65R rapidly increased after the introduction of TDF in clinical practice [3]. It is noteworthy that this follow-up study showed a decrease in the rate of K65R in isolates from patients who experienced failure of therapy with TDF, from 17% of isolates in 2004 to 3.6% of isolates in 2005 to 0% of isolates in 2006. This decrease occurred despite a relatively elevated and stable rate of prescription of TDF over the course of the study period. The main determinant of selection of K65R in our study was the coadministration of didanosine or abacavir. In fact, the high incidence of K65R in earlier years could be directly linked to widespread prescription of the combination of TDF plus didanosine at our institution, which peaked in 2003 at ∼35% of all patients receiving antiretroviral therapy. The coadministration of TDF plus didanosine was popular at that time because of its simplicity (1 pill each administered once per day), relatively good gastrointestinal tolerance, and expected avoidance of overlapping resistance. This attractiveness, however, soon disappeared when unexpected and seemingly parodoxical decreases in CD4+ cell count [9], mitochondrial toxicities (in- cluding pancreatitis), loss of body weight, and increased risk of hyperglycemia and diabetes [10] began to be reported. Furthermore, an open-label study was prematurely interrupted when a high rate of virological failure was noticed in drugnaive patients receiving TDF plus didanosine [11]. All patients in that study harbored viruses with M184V at the time of viral rebound, and one-half of those patients had virus with the K65R mutation. Similar results were obtained using the combination of TDF plus abacavir plus lamivudine in drug-naive individuals [12]. Both cross-resistance driven by selection of K65R and intracellular interactions between TDF and either didanosine and abacavir explained all of these findings. Although this knowledge has altered the use of TDF, there is no doubt that the availability of the coformulation of TDF with emtricitabine in a single pill has made the continuous use of TDF very attractive. In our study, this change in the use of TDF within the past 2 years has been associated with a dramatic reduction in the incidence of K65R. It should be noted that the most prevalent pattern of TDF resistance in our study was the presence of ⭓3 TAMs including Figure 2. Proportion of different tenofovir (TDF)–associated resistance mutations in virus obtained from 374 patients who experienced virological failure of TDF-containing regimens. Ins, insert; TAM, thymidine-associated mutation. 1784 • CID 2008:46 (1 June) • HIV/AIDS Table 2. Predictors of K65R in the multivariate analysis. Variable Antiretroviral drug Tenofovir Didanosine Abacavir Lamivudine Stavudine Resistance mutation Acknowledgments OR (95% CI) P 23.2 (9.8–54.8) 5.2 (2.6–10.6) .001 .001 4.1 (2.0–8.6) 1.4 (0.6–3.1) .001 .419 0.94 (0.3–3.1) .930 K70E 1.3 (0.1–14.4) .844 M184V a TAM 3.8 (1.9–7.8) .001 0.4 (0.3–0.5) .001 NOTE. TAM, thymidine-associated mutation. a OR is given per no. of TAMs. M41L and/or L210W. This is mainly attributable to the fact that most patients who experienced failure of TDF therapy had previously been exposed to zidovudine and/or stavudine. An inverse correlation between the presence of TAMs and K65R has already been shown [2, 3], and patients taking zidovudine in combination with TDF generally do not develop infection with virus that has the K65R mutation. In our study, most failures of TDF therapy in recent years occurred in subjects with virus that carried multiple TAMs; therefore, K65R is no longer a major concern. Other potential changes associated with TDF resistance, such as inserts at codon 69 or K70E, are very rare and are generally seen in patients with virus that harbors multiple TAMs or K65R, respectively. In summary, selection of virus with K65R in patients with HIV infection who experience failure of antiretroviral therapy has significantly decreased in recent years (at present, to !1% of patients receiving HAART), despite a relatively high and stable rate of prescription of TDF as part of antiretroviral regimens. A wiser use of TDF and, in particular, avoidance of coadministration with didanosine seem to explain this observation. Financial support. Fundación Investigación y Educación en SIDA, Instituto de Salud Carlos III-Redes Tematicas de Investigacion Cooperativa (RD06/006), Agencia Lain Entralgo, and Fondo de Investigaciones Sanitarias (projects CP06/00284 and PI06/1826). Potential conflicts of interest. All authors: no conflicts. References 1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents. Department of Health and Human Services. December 1st 2007. Available at: http://www.aidsinfo.nih.gov/contentfiles/adult andadolescentgl.pdf. Accessed December 2007. 2. Miller M. K65R, TAMs and tenofovir. AIDS Rev 2004; 6:22–33. 3. Valer L, Martin-Carbonero L, de Mendoza C, Corral A, Soriano V. Predictors of selection of K65R: tenofovir use and lack of thymidine analogue mutations. AIDS 2004; 18:2094–6. 4. Miller M, Margot N, Lu B, et al. Genotypic and phenotypic predictors of the magnitude of response to tenofovir disoproxil fumarate treatment in antiretroviral-experienced patients. J Infect Dis 2004; 189: 837–46. 5. Barrios A, de Mendoza C, Martin-Carbonero L, et al. Role of baseline HIV genotype as a predictor of viral response to tenofovir in heavily pre-treated patients. J Clin Microbiol 2003; 41:4421–3. 6. Delaugerre C, Roudiere L, Peytavin G, Rouzioux C, Virad J, Chaix M. Selection of a rare resistance profile in an HIV-1 infected patient exhibiting a failure to an antiretroviral regimen including tenofovir DF. J Clin Virol 2005; 32:241–4. 7. Johnson V, Brun-Vezinet F, Clotet B, et al. Update of the drug resistance mutations in HIV-1: 2007. Top HIV Med 2007; 15:119–25. 8. Margot M, Lu B, Cheng A, Miller M, and the Study 903 Team. Resistance development over 144 weeks in treatment-naı̈ve patients receiving tenofovir disoproxil fumarate or stavudine with lamivudine and efavirenz in the study 903. HIV Med 2006; 7:442–50. 9. Barrios A, Rendon A, Negredo E, et al. Paradoxical CD4+ T cell decline in HIV-infected patients with complete virus suppression taking tenofovir and didanosine. AIDS 2005; 19:569–75. 10. Garcia-Benayas T, Rendon A, Rodriguez-Novoa S, et al. Higher risk of hyperglycemia in HIV-infected patients treated with didanosine plus tenofovir. AIDS Res Hum Retroviruses 2006; 22:333–7. 11. Jemsek J, Hutcherson P, Harper E. Poor virological responses and early emergence of resistance in treatment-naive HIV-infected patients receiving a once daily triple nucleoside regimen of didanosine, lamivudine and tenofovir DF [abstract 51]. In: Program and abstracts of the 11th Conference on Retroviruses and Opportunistic Infections, 8–11 February 2004 (San Francisco). 12. Gallant J, Rodriguez A, Weinberg W, et al. Early virologic nonresponse to tenofovir, abacavir, and lamivudine in HIV-infected antiretroviralnaive subjects. J Infect Dis 2005; 192:1921–30. HIV/AIDS • CID 2008:46 (1 June) • 1785