The Verizon Minority Male Makers Program
Anuncio

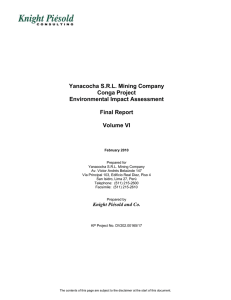
SUMMER STE M PROGRAM The Verizon Minority Male Makers Program-Directed by the Jun e 27 th to July 22 nd University of the District of Columbia The Verizon Minority Male Makers Program-Directed by the University of theDistrictofColumbiaisofferingafreeall-expensespaid4-weekintensive summer program designed to engage students in high quality, hands-on learning in Science, Technology, Engineering andMath (STEM) in order to increaseaccesstoSTEMfocusedcareersandhighereducation.Inaddition tothesummerprogram,studentswillreceiveamentorandparticipatein STEMworkshopsduringtheacademicyearatUDCandhostsitesacrossthe District! ForMoreInformation Contact Dr.JamesMaiden 202274-5768 [email protected] TheprogramisforyoungmalesofAfricanAmericanandHispanicdescent in grades 6th– 8th. Those selected will have the opportunity to learn 3D printing,Appdevelopment,androbotics.Therewillbecompetitions,prizes andexcitingfieldtrips. Give your child the opportunity to excel in the STEM area by receiving advance training from UDC academic leaders in the field. The Verizon MinorityMaleMakersprogramwascreatedbyVerizon,andisdirectedby theUniversityofDistrictofColumbia. aim m a r g l oo h sc D e h3 l l dd oug goa y i m hr e en b y t h t i t or ers ly, ty m n of mi mak ate ori s n e n io b l nd ltim m i t a a a en rs nt. U n of d ov or n o o f n s t eat pme ra tio y a e in res m r a i e c e lo ne log ld th utu m a om dev ge hno bui er f r og b ec pp new tec to ig ht r a s p e s to n d er a long kill e br ies. h T le n a ow ife p s at m il ma sig mp m l shi cre r fa r e i e e o d to th n eu d t the g s i vin re an nd p i g tre row s a e e n mor e lv to ems th T di he m sc cu od ip rr el lin icu lin es lu g, : a m de pp wi s i d ll c gn es o an ign ver d an a pr d ra in d ng tin ev e g; el of an op ST d me EM ro n bo t; 3 t ic D s. h t es o td ? a Wh ieve ach o t o r p e W ob h a ta tsk in il ? ls w ill th e st ud en ts Part icipa nts: A frica n A m erica n a n d Hisp Grad an i c es:6 th Mid t h r o dleS D a te u g h th ch oo :Jun 8 e27 th lBo ys t 4 W h r o eeks ugh July -M 22 nd ond ayth Tim roug Cu r r e:9: hFr iculu 3 iday 0 a m:R m to obo 3 : 30p Co l l tics, m ege Ap p Rea D evel dine opm ssan e n t, dEn 3 D tr e p Prin rene ting uria Field l Wor Trip ks h o s ps Me n torin Free M a g th T utor ingD urin Lu n c gSch h I n ool *Met clud r or a ed ilCa *T r a rdsw velI illbe nclu pro vide ded dto p artic ipan t swh one edt rans p or t atio n. REGISTRATIONFORM Theselectedparticipantswillattendtheprogramaccordingtothefollowingschedule: ProgramrunsJune27ththroughJuly22nd-MondaythroughFriday,9:30am–3:30pm Participationintheprogramisvoluntary.Ifyourchildisselected,heisexpectedtoattendeverydayfor the full four weeks. This packet contains the forms that must be completed and returned before the studentwillbeallowedtoattendsummerprogram. 1. 2. 3. 4. 5. 6. StudentInformation ParentalConsent,Release,HoldHarmlessandAuthorizationToReproducePhysicalLikeness VerizonGeneralReleaseFrom ProgramEvaluationandResearchReleaseForm ParticipantMedicalReleaseForm Field Trip Release Form –(A Field Trip Release Form will be provided prior to the date of the fieldtrip) PleasemakesurethatallfiveformsarecompletedandreturnedtousbyJune15th.Completedforms maybemailed,faxed,oremailtotheattentionof: Dr.JamesMaiden AssistantDeanofStudentAffairs TheUniversityoftheDistrictofColumbia 4200ConnecticutAvenue,NW Building41,Suite405 Washington,DC20008 [email protected] Fax:202274-5589 Phone:202274-5768 1. STUDENTINFORMATION Pleasemakesuretocompleteallrequiredinformationandprintclearlyonthisform.Missinginformation may cause delays in processing your child’s application and could cause him not to be eligible for the program. ParticipantInformation FirstName:________________________MiddleInitial_____LastName:___________________________ Phone:______________________Email:_____________________________________________________ Homeaddress_________________________________City________________State___Zip____________ School:_____________________________________________________Grade(asofFall2016):_______ Birthdate:_____________________ Ethnicity:(Checkone)___Black/AfricanAmerican ___Hispanic/Latino T-ShirtSize:(Checkone) YouthSize:___SM___MED___LG Parents/GuardianInformation Parents/GuardianFirstName:_________________MiddleInitial____LastName:___________________ Primarycontact:________________________Relationshiptoparticipant:_________________________ Homeaddress(Ifdifferent)____________________________City_________________________________ State__________Zip____________ CellPhone:___________________________Email:___________________________________________ Secondarycontact:_______________________Relationshiptoparticipant:_________________________ CellPhone:___________________________Email:___________________________________________ IconfirmthatIamtheParent/Guardianofthestudentparticipatingintheprogram: ______________________________________________________________________________________ Parent/guardian’snameandsignature Date 2.CONSENT,RELEASE,HOLDHARMLESSANDAUTHORIZATIONTOREPRODUCEPHYSICALLIKENESS I grant permission for my son (Please Print) _______________________________________________ to participateinTheVerizonMinorityMaleMakersProgramsummerprogram. Iunderstandthatinordertoparticipateinthisprogram,mysonmustabidebytheestablishedrulesand codesofconductestablishedbytheprogramstaff.TheVerizonMinorityMaleMakersProgramreserves the right to dismiss a child from the program due to that child's disruption of the program, failure to followsafetyorprograminstructions,andanyotherdisruptivebehavior. I understand and agree to assume any and all risks associated with the summer program activities. I understand that even with careful supervisions, accidents can occur. I recognize this risk and agree to release and forever discharge all the volunteers, staff and the schools where such activities take place fromanyandallclaims,demands,damages,actions,causesofaction,orsuitsofanykindornature,and particularly on account of all injuries, both to person or property, at any time or any place relating to participationintheprogram. ______________________________________________________________________________________ Parent/guardian’snameandsignature Date 3.GENERALRELEASE I grant Verizon Communications Inc., its subsidiaries, successors, assigns, and licensees (collectively “Verizon”) the following rights: 1.IgrantVerizontherighttotakephotographsandvideosofmeandmylikenessandrecordorotherwisetakemyvoicefor testimonialsandotherstatements(“Photography”)onthedateandatthelocationlistedbelow. 2.IalsograntVerizontherighttoeditandusethePhotographyinanywaywhatsoever,foranypurpose,andinanymanner andmedium,includingbutnotlimitedto,advertising,publicityorpromotionalmaterial,inprint,video,television,radio,orany othermedia,electronicorotherwise,includingwebsitesandtheInternet,atanytimeortimesthroughouttheworld,touse quotationsandsoundtrackrecordingsofmeormyvoice,includingtherighttosubstitutethevoiceofanotherperson(s)formy voice, to use my name or a fictitious name and biographical and other information, accurate or fictitious, concerning me in connectionwiththeuseofthePhotography. 3.IwaiveanyrighttoinspectorapprovethePhotographyorhowthePhotographyisusedandfurtherwaiveanyclaimthatI mayhavewithrespecttoitsuse. 4.IacknowledgethatIwillnotreceiveanycompensationotherthananypublicitythatImayreceiverelatingtotheuseofthe Photography. 5. I forever release and discharge, and agree to hold harmless Verizon and its directors, officers, agents, employees, shareholdersandrepresentativesfromanyandallliabilityforanyviolationofanypersonalrights(includingrightofprivacyand rightofpublicity),intellectualpropertyrightsoranyotherrightswhichImayhavearisingoutoforinconnectionwithVerizon’s useofthePhotography 6.IrepresentandwarrantthatIamoffullageandhaveeveryrighttocontractinmyownnameintheaboveregard.This agreementshallbebindinguponme,myheirs,legalrepresentativesandassigns. Locationanddate:_____________________________________________________________________ Iherebyagreeandconsent: PrintedName Signature Address Date Ifaminor:Iamthe(parent/legalguardian)ofthenamedminor.Iagreeandconsenttotheforegoingonbehalfoftheminor andpersonallyjoininthewarrantiesandrepresentationsabove.IalsoagreetoindemnifyandholdharmlessVerizonagainst anyclaimstheminormaymakeasaresultofVerizon’suseofthePhotographyasdescribedabove. PrintedNameof Minor PrintedNameof Parent/LegalGuardian SignatureofParent/Legal Guardian Address Date 3.Exenciónderesponsabilidadgeneral Pormediodelpresente,yo,elabajofirmante,otorgolossiguientesderechosaVerizonCommunicationsInc.,140 WestStreet,NewYork,NewYork10007,sussubsidiarias,sucesores,cesionariosyconcesionarios(colectivamente, “Verizon”): OtorgoaVerizonelderechoylaautorizaciónirrevocablesyabsolutospararegistrarmiimageny/omivozmediantefotografíafija,película, cintadevideo,grabacionesdesonidosocualquierotromedio(enadelante,“fotografía”)enlafechayellugarquesemencionanmás adelante. TambiénotorgoaVerizonelderechoaeditarsegúnsucriterio,usar,publicar,distribuir,exhibir,obtenerdichafotografíayotorgarlicencias deellaaterceros,demaneratotaloparcial,individualmenteojuntoconotrasfotografías,imágenesocualquiermaterialsujetoaderechos deautor,concualquierfinalidad,decualquiermanerayporcualquiermedio,comomaterialesdepublicidad,propagandaopromoción,entre otros,enformaimpresa,porvideo,televisión,radioocualquierotromediodecomunicación,pormedioselectrónicosodeotramanera, comositioswebeInternet,encualquiermomentoyentodoelmundoaperpetuidadsinlaobligacióndeinformarmealrespecto,aobtener derechosdeautordedichafotografíaensupropionombreodeotramanera,ausaroautorizarelusodecitasygrabacionesdesonidosmíos odemivoz,incluidoelderechoareemplazarlavozdeotrapersonaodeotraspersonaspormivoz,ausarminombreounnombreficticioe informaciónbiográficaodeotrotipo,precisaoficticia,respectodemipersonaorelacionadaconelusodedichafotografía. Pormediodelpresenterenuncioatododerechoarevisaroaprobarlafotografíaoelmaterialeditorialoimpresoquepuedautilizarsejuntocon ellos;asimismorenuncioacualquierreclamaciónquepudieratenerconrespectoalusoeventualalquepudieranestarsujetos, independientementedequeyotengaonoconocimientodeluso. AceptoqueVerizon,olosagentesdeVerizon,poseenlatitularidaddelosderechosdeautorsobrelafotografía.Sirecibieraunacopia impresa,ennegativoodeotrotipodedichafotografía,nopodréautorizaraningunaotrapersonaaquelause. Pormediodelpresentedeclaroygarantizoqueestaasignacióndederechosnocontradicedeningúnmodocualquiercompromisoqueyo tengaactualmente.Hastalafechanoheautorizado(conunaautorizaciónquesigaenvigor),niautorizarénipermitiréelusodeminombre, voz,cita,fotografíaoimagenenrelaciónconlapublicidadylapropagandadecualquierproductooservicioquepertenezcaalacompetencia oqueseaincompatibleconlosproductososerviciosqueofreceVerizon. Aceptoquenorecibirécompensaciónalgunaporotorgarlosderechosincluidosenelpresentedocumento. Pormediodelpresente,eximoyexoneroparasiempreyaceptolibraraVerizonysusdirectores,directivos,agentes,empleados,accionistas yrepresentantesdetodaresponsabilidadcausadaporlaviolacióndelosderechosindividuales(incluidoelderechoalaprivacidadyel derechoalapropiaimagen),losderechosdepropiedadintelectualocualquierotroderechoquepudierateneryquesurjadelusoporparte deVerizondelafotografíatalcomosedescribióanteriormente,oestérelacionadocondichouso,entrelosqueseincluyenerrores,aspecto borroso,distorsión,alteración,ilusiónópticaoauditivadelafotografía. Pormediodelpresentedeclaroygarantizoquesoymayordeedadyquetengoelderechodecelebrarelcontratoconrespectoaloanterior ennombrepropio.Elpresenteacuerdoserávinculanteparamí,misherederos,representanteslegalesycesionarios.Asimismodeclaroque heleídoestaExenciónderesponsabilidadgeneralantesdefirmarlayquecomprendosustérminos. Lugaryfecha:______________________________________________________________________________________________________ Título y n.° de proyecto: ______________________________________________________________________________________________ Información y firma de la persona fotografiada: Nombre (en letra de imprenta) Firma Dirección Fecha En caso de ser menor de edad: Soy (el padre/la madre/tutor legal) del menor indicado a continuación. Acepto la información precedente en nombre de dicho menor y personalmente adhiero a las declaraciones y garantías expuestas anteriormente. Asimismo, acepto indemnizar y librar de toda responsabilidad a Verizon con respecto a las reclamaciones que el menor pudiera hacer como resultado del ejercicio que Verizon haga 4.PROGRAMEVALUATIONANDRESEARCHRELEASEFORM The Verizon Minority Male Makers Program evaluates all its programs to make sure that they are effective, and to improve them, as needed. The evaluations and results are reviewed by those who oversee the program. The evaluations and results may also be used for scholarly research to increase minoritymales’entranceintotheSTEMfield. During the time your son is in The Verizon Minority Male Makers Program, he may be observed by evaluatorsandresearchersduringdifferentprogramactivitiesandmaybeaskedtogivehisfeedbackand opinionsinresponsetoquestionnairesorsurveys,infocusgroups,and/orininterviews. Your child’s participation is VOLUNTARY; he does not have to participate in these activities, and can choosenottoanswercertainquestions,ordecidenottoparticipate,orwithdrawfromparticipationat anytime. Theseevaluationassessmentsarenotanonymous,soyourchild’snamewillbeincludedontheformsthat areusedfortheevaluation(s);however,allinformationandresultswillbekeptstrictlyCONFIDENTIALand personal data will not be stored. Information identifying your child’s name will be removed before the results are analyzed and given out. Participants’ names will never be used in any report or publication. DatasharedwithVerizonwillbeinaggregateandnoindividualleveldata(oridentifyinginformation)will beshared. Finally, The Verizon Minority Male Makers Program reserves the right to use personal information (for example, permanent address, phone number, and/or email address) to contact participants after the program to gather information about their career or educational successes. Participants’ personal informationwillneverbedistributedoutsideofTheVerizonMinorityMaleMakersProgram–Directedby TheUniversityoftheDistrictofColumbia;willbekeptcompletelyconfidential;willbeusedbyauthorized personnelonly;andwillbestoredinpasswordprotectedandsecureserversordatabases. If you have any questions about this evaluation or about evaluation participants’ rights, please contact JamesMaiden,[email protected]. ByauthorizingyourchildtoparticipateinTheVerizonMinorityMaleMakersProgram,youareagreeingto the contents of this parental permission form – and indicating that you have read and understand the information above and allow your child to participate in the evaluation part of this program. When evaluationassessmentsarepresentedtoparticipantsintheprogram,yourchildwillbeinformedabout theevaluationstudyandabouthisrightsasaparticipant.Atthattimeyourchildwillbeaskedtoprovide hisagreementtochoosetoparticipateintheassessment. ______________________________________________________________________________________ Parent/guardian’snameandsignature Date 5.PARTICIPANTMEDICALRELEASEFORM-A NameofChild’sPhysician_________________________________________________________________ PhysicianPhone________________________________________________________________________ MedicalInsuranceCo._______________________________Policy/Group_________________________ Does the participant have any health conditions (i.e. allergies, chronic conditions), prescribed medications,orspecialcircumstances(i.e.religiousconvictionsorlegalarrangements)thatweshouldbe awareof? (Checkone)___NO___YES Ifyes,pleaseexplainonback. Pleasealsolistanymedication(s)theparticipantwillrequire(prescribedornot). ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ Intheeventofanemergency,whenparentsoremergencycontactscannotbereached,TheVerizon MinorityMaleMakersProgramhasmypermissiontotakemychildtothenearesthospital.(Checkone) ___NO___YES Pleaseprovidetheinformationofaresponsibleadultwhomwecancontactinanemergencyifweare unabletocontactyou. ______________________________________________________________________________________ Name Relationship Homeaddress_____________________________________City_________________________________ State__________Zip____________ DayandEveningphone(d)____________________________(e)_________________________ Email________________________________________ 5.PARTICIPANTMEDICALRELEASEFORM-B I/We certify that the participant is in good health and hereby authorize the directors of The Verizon Minority Male Makers Program to act for me/us, according to their best judgment, in any emergency requiringmedicalattention.I/Weunderstandandagreethatinstructors,counselors,andstaffmayneed to contact appropriate emergency medical providers regarding said minor. I/We give consent for any medicaltreatment(i.e.,diagnostic,therapeutic,andsurgicalprocedures)thatsuchmedicalprovidersmay deemnecessarywiththeunderstandingthatthecostofanysuchtreatmentwillbemy/ourresponsibility. I/We understand that my/our consent will allow procedures to be promptly carried out so that no unnecessary delays will occur with treatment. No operation will be performed, except in extreme emergency,withoutme/usbeingcontactedandfullyinformedandconsentobtained. ______________________________________________________________________________________ Parent/guardian’snameandsignature Date 6. FIELDTRIPRELEASEFORM (AFieldTripReleaseFormwillbeprovidedtoparentspriortothedateofthefieldtrip) Mychildhaspermissiontoparticipateinfieldtripswithchaperones,forsummerprogramactivities. ______________________________________________________________________________________ Parent/guardian’snameandsignature Date