negative feelings and psychological processes in families with
Anuncio

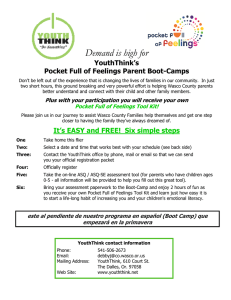
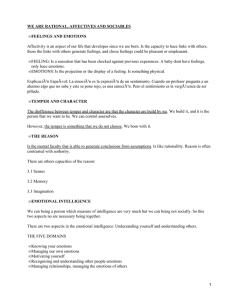
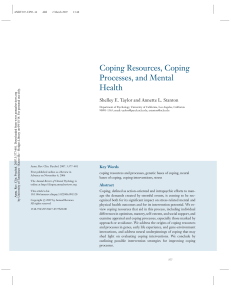
NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION RESUMEN Las enfermedades cardiacas congénitas (ECC) tienen un fuerte impacto en la familia. La investigación interesada en la salud de los menores en relación con ECC ha enfatizado la importancia de los sentimientos de los progenitores, dado que su ajuste a la situación afecta la calidad de vida del menor y la familia. El objetivo de este trabajo fue analizar los sentimientos negativos más significativos relacionados con las necesidades psicológicas experimentadas por los progenitores durante el diagnóstico y la hospitalización. El objetivo específico fue analizar la relación entre sentimientos negativos, por un lado, y procesos cognitivos, comportamientos y estrategias de afrontamiento, por otro. 347 progenitores completaron escalas de medida de sentimientos negativos generales, específicos y estrategias de afrontamiento, midiendo tanto estrategias actuales como su utilidad percibida. Las escalas fueron completadas para las fases de diagnóstico y hospitalización. El temor al pronóstico y a la recuperación son preocupaciones comunes durante ambas fases y se relacionan con sentimientos negativos generales y específicos. Sin embargo, se detectaron diferencias en relación a las estrategias de afrontamiento, que se centran en las emociones durante el diagnóstico y en los problemas durante la hospitalización. El apoyo social profesional surge como un factor clave para manejar sentimientos negativos en ambas fases. El carácter exploratorio de este estudio sugiere la necesidad de tratar con cautela los resultados. Son precisas más investigaciones para incrementar el conocimiento y establecer relaciones causales entre los sentimientos negativos, por un lado, y el apoyo social, las estrategias de afrontamiento y los procesos cognitivos, por otro. Conceptos como desesperanza y sentido de control pueden ser explicaciones apropiadas para explicar el ajuste emocional de los progenitores ante las ECC. Palabras clave: Enfermedad cardiaca congénita, sentimientos negativos, ajuste parental, afrontamiento, apoyo social. CORRESPONDENCIA Ana Barrón1 Esteban Sánchez2 Isabel Varela3 Andrés Arias4 1.Complutense University of Madrid. Faculty of Psychology, Campus de Somosaguas, 28223 Pozuelo (Madrid) SPAIN. 2.Institute for Advanced Research University of Tarapacá (Arica, Chile). 3.Faculty of Psychology University Alfonso X El Sabio. 4.Faculty of Social Work Complutense University of Madrid. ABSTRACT Correo autor: Congenital heart disease (CHD) has a strong impact within the family. Researchers interested in child health [email protected] outcomes in relation to CHD have highlighted the importance of parental feelings, with their adjustment to the situation affecting quality of life for child and family. The objective of this work was to analyze the most significant negative feelings related to the psychosocial needs experienced by parents during diagnosis and hospitalization. The specific aim was to analyze relationships among negative feelings and cognitive process, behaviors, and coping strategies. 347 parents whose child was diagnosed with CHD completed scales measuring generalized and particular negative feelings and coping strategies, measuring both real strategies and their perceived usefulness. The scales were completed for diagnosis and hospitalization. Fear of prognosis and recovery are common worries during both phases and relate to generalized and particular negative feelings. However, differences appear concerning coping strategies, which are focused on emotions in diagnosis but problems in hospitalization. Professional social support emerges as a key factor to manage negative feelings in both phases. The exploratory character of this study demands that its findings be treated cautiously. Further research is required to increase the knowledge base and establish causal relationships among negative feelings, on one hand, and social support, coping strategies and cognitive processes, on the other. Concepts such as hopelessness and control are suggested as appropriate explanations for parents’ emotional adjustment to child CHD. Keywords: Congenital heart disease, negative feelings, parental adjustment, coping, social support. BACKGROUND Congenital heart disease (CHD) is a chronic illness, meaning rates and life expectancy. children and their families must learn to live with a complex situation on a daily and permanent basis. Advances in medicine and surgical treatments have increased survival • Nowadays, child heart disease is the congenital pathology of greatest incidence in Spain, affecting Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 31 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN an estimated eight in every thousand live births. isolation, etc.). Most sufferers need treatment during the first year of their life. In most cases there is a medical or surgical In terms of well-being, the most widely mentioned feeling solution, but affected children will need follow-up (1) and was uncertainty about the future (71%). However, 93% must adapt to their situation throughout their lives of parents were hopeful regarding the illness’ evolution. (2) . CHD diagnosis has a strong impact within the family. Recent studies (6) offer similar results. Moreover, heart disease usually triggers social, work, and family conflicts (3). Families go through different phases in accepting the illness. An initial phase of emotional crisis involves several Heart disease can affect the integrity of the family unit. It feelings: anger, guilt, and incomprehension. There is then is important to understand how families experience this a phase of adaptation to the new reality, accompanied by process in order to maintain or restore the family balance sadness and depression. At this time, families begin to . The main aim of any intervention is therefore to increase reorganise family life. The final phase is stability, where the quality of life of affected children from a bio-psycho-social family accepts the new situation, copes with the problem, perspective . and finds an appropriate balance between the requirements (4) (5) of the illness and those of the family (1). In their pioneering study, Appley, Barbour, and Westmacott (6) demonstrated different dysfunctions within the family Previous studies show that the main problems encountered environment following cardiac disease diagnosis. Their concerning the hospital system are sample constituted 100 parents of children affected by about the illness, ignorance about medical treatments, CHD. Of those parents, 54% suffered a significant family difficulties related to communication of medical information, imbalance, such as changing jobs or moving house. lack of knowledge about prognosis and evolution of the Financial problems arose in 45% of cases, while 36% illness, disorientation in the hospital, and fear of medical experienced changes in social lives (holidays, parties, staff. Llopis Cañamera (8) carried out research with parents etc.). Regarding initial responses, 39% of mothers suffered of affected children aimed at discerning the main concerns a “shock” reaction and were more emotionally affected of families, showing that both parents exhibited feelings of than fathers. Adaptation to the new situation then occurred, guilt and impotence, particularly upon diagnosis. (7, 13, 16, 25) uncertainty but 68% of mothers and 43% of fathers reported an unsatisfactory relationship with the child. Home return involves changing lifestyles, adopting new roles, etc. Medical supervision disappears and considerable In a recent study, Montalvo, Romero, and Florez (2011) uncertainty arises regarding the appropriate level of reviewed different dysfunctional areas regarding childcare. physical activity for the child. In this situation, services In physical terms, 36.3% of parents reported changes focused on informing, orienting, and supporting the parents in their sleep habits and 30.8% fatigue. Overall, most are necessary (9). respondents (64.8%) evaluated their physical health as poor due to their child’s illness. In psychological terms, Parents play a key role throughout, having to transmit a parents reported fear of relapse, emotional disturbance sense of security and trust and ensure their children live due to diagnosis and treatment, etc., and 17% of parents as normally as possible within the limits imposed by the rated their psychological state as poor (financial burdens, illness, while avoiding over-protectiveness Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 32 (10) . To achieve NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN this balance, parents must be properly informed and receive adequate medical, psychological, and social support throughout the adaptation process 1. Development of questionnaires to assess needs in . Moreover, health three key phases: hospitalisation, diagnosis, and professionals must know the main needs and concerns of home return. The present article focuses exclusively parents in order to plan suitable interventions on diagnosis and hospitalisation, since the amount of (15, 22, 30) (24, 29) . information obtained exceeded the recommended size To analyse these issues in depth, research was designed and conducted in collaboration with “Fundación Menudos Corazones”. As mentioned, there are few studies in which of a single work. 2. Provision of questionnaires to a sample of affected families. issues such as concerns, family psychosocial adjustment, 3. Analysis and interpretation of data and results in order and return to daily life are assessed in reliable empirical to improve existing support or design new means of research. This research gap is remarkable given that support to satisfy needs of affected families. interventions carried out in Spain with affected families are not institutionalised, but rather supported and conducted 347 parents completed the questionnaires (15.9% men and by private associations, including “Fundación Menudos 84.1% women). Mean age was 39 years (SD= 6.33). Most Corazones” (nationwide), “Todo Corazón” (in Murcia), participants were married (89.7%), and 66.4% had to move “Asociación de Cadiopatías Congénitas” (the Balearic because of their child’s illness. Mean age of children was Islands), or “Associació d’Ajuda als Afectats de Cardiopatíes between 0 and 5 years (52%) and between 6 and 10 (23.3%). Infatils” (Catalonia). Such interventions are not grounded in Concerning child gender, the final sample comprised research focused on the specific needs of those families 55.4% boys and 44.6% girls. Regarding educational level in different coping stages, despite this information being a of parents, the sample was: 18% primary education, 36% basic requirement for the proper design of any intervention secondary education, 45% higher education, and 1% program. without formal education. The overall objective of this work was to analyse the The Social Psychology Department at Complutense most significant negative feelings related to psychosocial University in Madrid designed the questionnaires (see needs and challenges for affected parents and families below). The administration of the questionnaire was in the diagnosis and hospitalisation stages of coping with supported by “Fundación Menudos Corazones” [“Small CHD. The specific aim was to analyse correlations among Hearts Foundation”], that granted access to participants. negative feelings and cognitive process (concerns), This support was a key factor, since the families facing behaviours, and coping strategies (seeking of social a traumatic event like the one considered in this piece of support and information). The final goal was to improve research are likely to express refusal. This circumstance existing interventions or design new ones engineered to poses a clear difficulty for researchers, fortunately satisfy families needs. overcome through the action of a close a supporting agent METHOD for the families. Once contacted, all participants in the study completed both the diagnosis and hospitalisation Participants and procedure. questionnaires as different phases of the present piece of Our research proceeded as follows: research. Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 33 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN Measures same situation, looking for health professional support Negative feelings such as psychologists, nurses, social workers, etc, being A questionnaire was developed to assess the affective at the hospital most of the time (H), looking for information component of families’ psychosocial needs. Since the study about surgical procedures (H), looking for information about did not seek to analyse depression in a clinical sense, a secondary effects and how to deal with them (H), denial, six-item instrument was developed. The feelings included distraction, free accommodation, financial support, and were sadness, fear, anguish, guilt, rage, and impotence. social worker guidance. The questionnaire differentiated A Likert-type scale was used to assess their intensity for actual behaviour and perceived usefulness of coping the respondent, based on previous research showing those strategies. feelings were the most frequently experienced among parents of children affected by CHD. This questionnaire In summary, the variables under study were: (1) negative was applied both in diagnosis and hospitalisation, the feelings, (2) worries/concerns (cognitive dimension), (3) internal reliability being α = 0.673 for diagnosis and α = actual coping strategies (behavioural dimension), and (4) 0.740 for hospitalisation. perceived usefulness of coping strategies. Concerns / worries To assess concerns and worries (the cognitive dimension RESULTS of the psychosocial needs), a specific questionnaire was developed for parents of affected children. As mentioned, Table 1 provides the descriptive statistics for the main study previous research shows that the most frequent worries variable, focusing on negative feelings. Since means for in both stages are: fear about prognosis, fear related to rage and guilt were much lower than for other variables, recovery, what to tell the child, how to talk with and treat these results were excluded in order to better analyse the the other members of the family, restructuring of family main feelings. life, possible financial problems, possible work problems, and home return. The internal reliability was α = 0.740 for Preliminary exploratory analyses were conducted to assess diagnosis and α = 0.748 for hospitalisation. whether any of the socio-demographic variables were associated with negative feelings. Potential relationships Coping strategies between generalised and particular negative feelings and The behavioural component of the psychosocial needs categorical variables were assessed using t-test (sex, relates to how parents cope with challenges directly related marital status, moving from home city, education, child to the stressful event. Specific items were developed for sex, and participation in a formal support program). Since diagnosis and hospitalisation, since previous research education was transformed into two dummy variables shows that situational challenges change depending on (secondary and higher education), t-test was considered the phase. Nevertheless, the structure of the questionnaire an appropriate analysis for this purpose. remained the same, including the following dimensions: seeking information, seeking social support, seeking Several significant differences were found for socio- professional guidance, and denial. Specifically, the items demographic variable in diagnosis. Sadness (t = 3.312; p included were: looking for medical information, looking < 0.05) and GNF (t = 2.605; p < 0.01) scores were higher for family support, looking for the support of people in the for females. Impotence was higher among single parents Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 34 NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN Tabla 1: Descriptive statistics for negative feelings variables. Potential Range Diagnosis Mean (SD) Hospitalisation Mean (SD) Sadness 0-4 3.62 (0.72) 3.49 (0.80) Fear 0-4 3.76 (0.54) 3.81 (0.48) Anguish 0-4 3.71 (0.60) 3.68 (0.62) Guilt 0-4 2.51 (1.16) 2.27 (1.16) Rage 0-4 2.93 (1.20) 2.73 (1.21) Impotence 0-4 3.62 (0.75) 3.45 (0.87) GNF 0-24 20.09 (3.21) 19.37 (3.49) GNF, generalised negative feelings. (t = 2.219; p < 0.05). Finally, respondents holding higher impotence. This statement applies to the different university qualifications scored lower in sadness (t = 2.302; dimensions considered in the questionnaire (cognitive p < 0.05), impotence (t = 2.539; p < 0.05), and GNF (t = processes, real coping strategies, and perceived usefulness 3.201; p < 0.01). of coping strategies) (tables not shown, available from correspondence author). During hospitalisation, females scored higher in anguish (t = 1.982; p < 0.05). Scores for respondents with higher Given these results and those for socio-demographic education were lower for sadness (t = 3.028; p < 0.01), variables, and the exploratory nature of our piece of fear (t = 2.010; p < 0.05), impotence (t = 2.609; p < 0.01), research, all the variables were incorporated in the next and GNF (t = 3.308; p < 0.01). Moreover, respondents analytical step (regression). Separate regression analyses that had participated in a support program scored lower in were performed to predict GNF and the main emotional impotence (t = 2.348; p < 0.05). dimensions considered in the questionnaire (sadness, fear, anguish, and impotence) for diagnosis and hospitalisation. Potential relationships among GNF, particular feelings, and continuous study variables were assessed using Regarding GNF, results for diagnosis and hospitalisation are Pearson correlations for common variables in diagnosis shown in tables 2 and 3 respectively. A number of variables and hospitalisation. For both diagnosis and hospitalisation, obtained significant coefficients for both stages, specifically a remarkable number of variables significantly correlated fear of prognosis and fear for recovery, which scores are with negative feelings of sadness, fear, anguish, and positively related to negative feelings. Moreover, a different Table 2: Multiple regression analysis assessing parents’ negative feelings in diagnosis. Variable B SE B β Age (respondent) 0.001 0.004 0.012 Sex (respondent) 0.130 0.068 0.094† Number of children 0.011 0.035 0.018 Marital status - 0.093 0.080 - 0.056 Move from home city - 0.084 0.054 - 0.078 Secondary education 0.070 0.070 0.067 - 0.054 0.070 -0.053 0.025 0.082 0.015 High education Intervention program Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 35 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN Child sex Position among siblings 0.014 0.049 0.013 - 0.033 0.044 - 0.042 0.216 0.048 0.238*** Worries (cognitive dimension) Fear of prognosis Fear for recovery 0.057 0.047 0.063* What to say the child 0.018 0.037 0.034 How to treat the child 0.067 0.038 0.132† Family life management 0.063 0.031 0.120 Financial problems 0.072 0.032 0.146* - 0.002 0.030 - 0.004 0.056 0.026 0.117* Look for medical information 0.041 0.042 0.061 Look for family support 0.011 0.038 0.019 Look for peers support - 0.036 0.038 -0.070 0.068 0.040 0.125† 0.016 0.050 0.020 - 0.025 0.042 - 0.046 Work problems Home return Real coping strategies Look for health professionals support Denial Information about free accommodation Information about financial support 0.129 0.053 0.190* - 0.042 0.049 - 0.064 Look for medical information - 0.059 0.041 - 0.088 Look for family support - 0.037 0.041 - 0.063 Social workers guidelines Perceived usefulness of coping strategies Look for peers support 0.032 0.039 0.062 Look for help professionals support - 0.081 0.039 - 0.155* Denial - 0.040 0.046 - 0.051 Information about free accommodation 0.023 0.032 0.049 Information about financial support 0.007 0.042 0.012 Social workers guidelines 0.039 0.042 0.066 Final R2=0.33; final adjusted R2=0.26; †P < 0.10, *P < .0.05, **P < 0.01, ***P < 0.001 Table 3: Multiple regression analysis assessing parents’ negative feelings in hospitalisation. Variable B SE B β Age (respondent) - 0.003 0.005 - 0.37 Sex (respondent) 0.067 0.075 0.046 Number of children - 0.013 0.040 - 0.020 Marital status - 0.105 0.088 - 0.060 Move from home city - 0.059 0.059 - 0.052 Secondary education - 0.029 0.077 - 0.027 High education - 0.156 0.078 - 0.146* Intervention program - 0.153 0.093 - 0.088 Child sex Position among siblings 0.026 0.054 0.024 - 0.010 0.050 - 0.013 0.057 0.055 0.160** Worries (cognitive dimension) Fear of prognosis Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 36 NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN Fear for recovery 0.144 0.067 0.120* What to say the child - 0.016 0.045 - 0.028 How to treat the child 0.107 0.046 0.194* Family life management 0.090 0.033 0.163** Financial problems 0.013 0.038 0.024 Work problems - 0.013 0.037 - 0.025 Feeding 0.012 0.029 0.022 Home return 0.035 0.033 0.063 Look for medical information 0.020 0.042 0.031 Look for family support 0.001 0.050 0.002 Real coping strategies Look for peers support Look for health professionals support Being in the hospital Denial Look for information about surgery Look for information about secondary effects Look for information about dealing secondary effects Information about free accommodation 0.032 0.044 0.060 - 0.032 0.046 - 0.054 0.037 0.044 0.056 - 0.038 0.041 - 0.063 0.041 0.052 0.068 - 0.038 0.064 - 0.064 0.110 0.058 0.190† - 0.044 0.042 - 0.087 Information about financial support 0.032 0.058 0.049 Social workers guidelines 0.052 0.056 0.079 Look for medical information - 0.067 0.053 - 0.095 Look for family support - 0.006 0.055 - 0.010 Look for peers support Perceived usefulness of coping strategies - 0.013 0.048 - 0.023 Look for health professionals support 0.003 0.042 0.005 Being in the hospital 0.008 0.042 0.013 Denial Look for information about surgery Look for information about secondary effects Look for information about dealing secondary effects Information about free accommodation 0.029 0.038 0.050 - 0.061 0.061 - 0.096 0.088 0.076 0.145 - 0.065 0.072 - 0.106 0.056 0.039 0.114 Information about financial support - 0.025 0.051 - 0.043 Social workers guidelines - 0.017 0.051 - 0.028 Final R2=0.31; final adjusted R2=0.21; †P < 0.10, *P < .0.05, **P < 0.01, ***P < 0.001 set of variables resulted in significant coefficients depending worries about how to treat the child and worries about family on the stage. For diagnosis, worries about financial problems life management. In addition, one demographic variable and home return, both correlated positively with scores for was related to negative feelings. Specifically, respondents negative feelings. Regarding actual coping strategies, a in the higher education group showed lower scores in the positive and significant coefficient was obtained for seeking GNF variable. financial support. Finally, concerning perceived usefulness Following the analysis for the GNF variable, separate of coping strategies, seeking professional support reduced analyses were conducted for four specific negative feelings: negative feelings. For hospitalisation, the main relationships sadness, fear, anguish, and impotence. As stated, all four involved positive regression coefficients being obtained for were measured in both diagnosis and hospitalization Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 37 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN (detailed tables showing the results obtained can be effects (actual behavior) (β = 0.248; p < 0.05) and obtained from the correspondence author). Again, worries position among siblings (β = 0.149; p < 0.05), with about prognosis obtained significant regression coefficients a negative coefficient for actual seeking of health for every negative feeling considered both in diagnosis professional support (β = 0.211; p < 0.01). and hospitalisation. Moreover, worries about the recovery • Impotence: For diagnosis, our results show a positive variable obtained significant coefficients for fear (β = 0.145; relationship with worries about home return (β = 0.198; p < 0.01) and impotence (β = 0.123; p < 0.05) in both phases, p < 0.001) and actual looking for medical information (β but for anguish this relationship was only observed for = 0.127; p < 0.05). However, the relationship is negative hospitalization (β = 0.196; p < 0.001). However, differences in the cases of those married (β = 0.139; p < 0.01) and in the regression equation were found among the specific the perceived usefulness of seeking health professional negative feelings, as described below. support (β = 0.153; p < 0.05). For hospitalisation, a positive regression coefficient was found for looking • Sadness: For diagnosis, women obtained higher for information about surgery (actual behavior) (β = scores (β = 0.110; p < 0.05) and perceived usefulness 0.183; p < 0.05), with negative regression coefficients of seeking health professional support diminished for those married (β = 0.130; p < 0.05) and participating sadness (β = 0.174; p < 0.05). For hospitalisation, in an intervention program (β = 0.137; p < 0.05). worries about how to treat the child obtained a positive correlation (β = 0.204; p < 0.05), while perceived usefulness of seeking information about surgery (β = DISCUSSION 0.198; p < 0.05) and higher education (β = 0.149; p < • 0.05) showed a negative relationship. Our results support previous findings about the challenges Fear: For diagnosis, a positive relationship was found posed by different phases when families face child CHD. with number of children in the family (β = 0.133; p < As stated, our research focused specifically on diagnosis 0.05), with negative correlations for moving away from and hospitalisation. Although there are common processes home city (β = 0.120; p < 0.05) and perceived usefulness for both phases, it is important to identify the particularly of seeking information about financial support (β = significant variables in each one, in order to offer cues for 0.143; p < 0.05). Regarding hospitalisation, positive improvement of intervention programs. regression coefficients were found for looking for • information about secondary effects (actual behavior) Commonalities: the key role of cognition (β = 0.278; p < 0.01), and negative coefficients for Our results highlight the importance of cognitive processes perceived usefulness of seeking medical information during diagnosis and hospitalisation. Specifically, two main (β = 0.211; p < .01), higher education (β = 0.217; p < worries pervade both stages, being significant for GNF 0.01), and being married (β = 0.132; p < 0.01). and almost every particular feeling: fear of prognosis and Anguish: For diagnosis, a positive relationship was fear for recovery. Although true that other variables are found with actual looking for family support (β = 0.152; significant in the regression analysis for GNF (for example, p < 0.05), and a negative one for perceived usefulness concerns about how to treat the child, home return, etc.), of looking for family support (β = 0.064; p < 0.05). For when considering the regression equations for particular hospitalisation, positive regression coefficients were feelings, only worries about prognosis and recovery remain observed for looking for information about secondary as key factors in both phases. Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 38 NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN emotions, while hospitalisation generates other demands Previous research demonstrates the relevance related with needing to improve the sense of control over of cognitive factors for parents facing CHD in a broad the situation. Previous studies offer contradictory results. sense. Our research is consistent with those findings, and (31) emphasises particular cognitive contents – those related health and adjustment among mothers of children affected with prognosis and recovery. by cystic fibrosis. Similarly, Davis et al. (1998) found the (3, 11, 27) Failed to find an association between locus of control for adjustment of parents of children affected by CHD was Differences: the specificity of coping processes unrelated to self-efficacy and locus of control. However, While it has been observed that commonalities are related recent theoretical and empirical developments on the role to cognitive processes, differences emerge regarding played by sense of control in psychosocial adjustment may coping processes. In this vein, important variations prove more efficient and specific in explaining parental between diagnosis and hospitalisation are detected in adjustment to children’s chronic illness. Particularly, coping strategies used by parents to confront stressful the hopelessness development of the classic learned situations. A clear tendency to use coping strategies helplessness theory (Abramson et al., 1995) should be oriented to managing emotions emerges as the most considered to account for the relation between emotional relevant to reduce negative feelings during diagnosis. adjustment and sense of control for parents facing the Most strategies relate to looking for social support, mainly stressful situation at hand. Control-based explanation is from social workers, psychologists, and family: basically, in this sense consistent with recent findings showing that emotional social support. Moreover, perceived usefulness parents of children affected by CHD frequently experience of this behavior correlates with lower scores for sadness, hopelessness feelings (20). anguish, and impotence. However, during hospitalisation this tendency changes and the more significant coping In their well-known article on the importance of social strategies focus on managing the problem. Specifically in support, Cohen & McKay (1984) proposed the stress- this phase, behaviors preventing negative feelings centre support matching hypothesis suggesting that support is around looking for medical information, such as looking for more likely to be beneficial when matched with the demands information about surgery and secondary effects. Again, of the stressor. This hypothesis finds support in later studies perceived usefulness of these strategies corresponds to (9, 17, 23) lower scores in different negative feelings (sadness and approach. In this vein, looking for information could be fear). This is consistent with previous studies considered a specific strategy based on social support – in (20) . . Our results seem to fit well with this theoretical this case, informational social support – which should be These findings are consistent with key theoretical models the best match with the demands posed in hospitalisation, of coping and social support . The classical model of since it involves surgery or medical procedures. The main advocates the contextual nature of sources of this kind of information during hospitalisation are Lazarus y Folkman (12) (28) coping strategies, with appraisal and coping emerging from surgeons, doctors, and health professionals. the interaction between situational demands and personal factors. Effectiveness of coping is defined by the match Sociodemographic variables. between real strategies and the specific demands posed Sociodemographic variables appear more important during by the situation. In our study, it seems diagnosis can elicit a hospitalisation, with higher education and marital status shock-like state best handled through strategies oriented to significantly related to GNF and to particular feelings Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 39 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN of sadness, fear, and impotence. This seems logical as parents at particular stages of coping with heart disease (24). these variables relate to differential access to important Further research is needed to design and develop effective coping resources: social and financial support, and ability interventions aimed at improving quality of life for affected to access and understand relevant medical information. families. Unmarried people may suffer greater task overload due to lack of partner social support; this may prove particularly important when other social support sources are limited. REFERENCES Participants with higher education are better equipped to cope both cognitively and practically with the challenges 1. AACI Asociación de Ayuda a las Cardiopatías Infantiles of this kind of situation, being better able to locate and de Catalunya. El niño con cardiopatía congénita en su understand medical information and confront challenges. entorno educativo, social y familiar. Madrid, España. People with higher education tend to enjoy better financial 2006. status, hence more easily obtaining specialist help when 2. Abramson L, Metalsky G, Alloy L. Hopelessness necessary. Moreover, this explanation is consistent with depression: A theory-based subtype of depression. attempting to control the situation, thereby avoiding Psychological Review. 1989; 96(2): 358-372. feelings of hopelessness. As stated, resources linked to 3. Graham T. Best Practices in Managing Transition to higher education and marriage probably provide a range of Adulthood for Adolescents With Congenital Heart resources that make it easier to develop problem-focused Disease: The Transition Process and Medical and coping strategies, allowing an increased sense of control. Psychosocial Issues: A Scientific Statement From the American Heart Association. Yearbook of Cardiology. 2012; 2012: 138-139. CONCLUSION AND LIMITATIONS 4. Apley J, Barbour R, Westmacott I. Impact of congenital heart disease on the family: preliminary report. BMJ. The exploratory and descriptive character of this study demands caution. Further research is needed to increase the knowledge base and establish causal relationships. 1967; 1(5532): 103-105. 5. Barrón A. Estrés, apoyo social y trastornos cardiovasculares. Jano. 2004; 67, 93-94. Following Wallander (1992), theoretical models testing 6. Bjorbækmo W, Engelsrud G. ‘I am almost like a fish’: proposed explanations should guide such research. Along an investigation of how children with congenital heart these lines, theory-grounded research should emphasise disease experience and perform movement in daily life. the roles of social support, coping strategies, and cognitive Child: Care, Health and Development. 2008; 34, 781- processes, within the context of concepts of hopelessness 788. and control, to explain the feelings parents experience. 7. Bragado C. Terapia de conducta en la infancia. Madrid: Fundación Universidad-Empresa; 1994. It is remarkable that peer support does not attain significance 8. Cohen S, McKay G. Social support, stress and the in our results. Yet although this may seem unexpected, it buffering hypothesis: A theoretical analysis. En: is in fact consistent with the proposed explanation, since Handbook of Psychology and Health (eds A. Baum, the usefulness of such support would be greater during S.E. Taylor & J.E. Singer). NJ, USA; 1984. p. 253-267. home return. Our results suggest the need for specific 9. Cutrona C, Russell D. Type of social support and interventions aimed at properly managing demands on specific stress: toward a theory of optimal matching. Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 40 NEGATIVE FEELINGS AND PSYCHOLOGICAL PROCESSES IN FAMILIES WITH CHILDREN AFFECTED BY CONGENITAL HEART DISEASE DURING DIAGNOSIS AND HOSPITALIZATION ARTÍCULO DE INVESTIGACIÓN En: Social support: An interactional view (eds. B.R. Sarason, I.G. Sarason & G.R. Pierce), John Wiley & Sons. Oxford, England; 1990. p. 319-366. Hague, The Netherlands; 1985. p. 391-414. 18. Lawoko S, Soares J. Distress and hopelessness among parents of children with congenital heart disease, 10. Davis C, Brown R, Bakeman R, Campbell R. parents of children with other diseases, and parents of Psychological Adaptation and Adjustment of Mothers healthy children. Journal of Psychosomatic Research. of Children With Congenital Heart Disease: Stress, 2002; 52(4): 193-208. Coping, and Family Functioning. J Pediatr Psychol. 1998; 23(4): 219-228. 19. Lawoko Soares J. Psychosocial morbidity among parents of children with congenital heart disease: 11. Doherty N, McCusker C, Molloy B, Mulholland C, A prospective longitudinal study. Heart & Lung: The Rooney N, Craig B, Sands A, Stewart M, Casey F. Journal of Acute and Critical Care. 2006; 35(5): 301- Predictors of psychological functioning in mothers 314. and fathers of infants born with severe congenital 20. Lawoko S. Factors influencing satisfaction and well- heart disease. Journal of Reproductive and Infant being among parents of congenital heart disease Psychology. 2009; 27(4), 390-400. children: development of a conceptual model based on 12. Folkman M, Lazarus R. Coping and emotion. En: Stress and coping, An Anthology (eds A. Monat & R.S. Lazarus). New York, USA: Columbia University Press; 1991. p. 207-227. the literature review. Scandinavian Journal of Caring Sciences. 2007; 21(1): 106-117. 21. Lazarus R, Folkman M. Stress, Appraisal, and Coping. New York, USA: Springer Publishing Company; 1984. 13. Galindo A. Proyecto de intervención psicológica en 22. Leon A, Wallenberg J, Holliker S. The Impact of Child las familias de niños con cardiopatías congénitas: Congenital Heart Disease on Parents of Very Young aplicación de un programa de relajación progresiva. Children: Considerations for Social Work Practice. Mapfre Medicina. 2006; 17, 38-46. Families in Society: The Journal of Contemporary 14. Gore S, Aseltine R. Protective processes in Social Services. 2013; 94(2): 129-135. adolescence: matching stressors with social resources. 23. Llopis J. Corazones de papel: patrones de cambio en American Journal of Community Psychology. 1995; 23, las familias con niños con cardiopatías congénitas. 301-327. Department of Social and Cultural Anthropology, 15. Harvey K, Kovalesky A, Woods R, Loan L. Experiences Autonomous University of Barcelona; 2011. of mothers of infants with congenital heart disease 24. McCusker C, Doherty N, Molloy B, Rooney N, before, during, and after complex cardiac surgery. Mulholland C, Sands A et al. A controlled trial of early Heart & Lung: The Journal of Acute and Critical Care. interventions to promote maternal adjustment and 2013; 42(6): 399-406. development in infants born with severe congenital 16. Hearps S, McCarthy M, Muscara F, Hearps S, Burke K, Jones B et al. Psychosocial risk in families of infants heart disease. Child: Care, Health and Development. 2010; 36(1): 110-117. undergoing surgery for a serious congenital heart 25. Montalvo A, Romero E, Flórez I. Percepción de la disease. Cardiology in the Young. 2013; 24(04): 632- calidad de vida de cuidadores de niños con cardiopatía 639. congénita. Investigación Educativa en Enfermería. 17. Hobfoll S. Limitations of social support in the stress 2011; 29: 9-18. process. En: Social support: Theory, research and 26. Rojas I. Evaluación de la capacidad cognitiva y applications (eds I.G. Sarason & B.R. Sarason). The comportamental de niños intervenidos de corazón. Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 41 BARRÓN A. ET AL. ARTÍCULO DE INVESTIGACIÓN Faculty of Psychology. Seville, Spain: University of Coping, and Family Functioning in the Psychological Seville; 2001. Adjustment of Mothers of Children and Adolescents 27. Salgado C, Carvalho Z, Haikel R, de Melo L, Lamy,. Pediatric cardiac surgery under the parents sight: a qualitative study. Revista Brasileira de Cirurgia Cardiovascular. 2011; 26, 36-42. 28. Moreno E. Collectivize Social Support? Elements for Reconsidering the Social Dimension in the Study of Social Support. Span j psychol. 2004; 7(02): 124-134. 29. Soulvie M, Desai P, White C, Sullivan B. Psychological distress experienced by parents of young children with with Cystic Fibrosis. J Pediatr Psychol. 1992; 17(5): 573-585. 32. Utens E, Versluis-Den Bieman H, Verhulst F, Witsenburg M, Bogers A, Hess J. Psychological distress and styles of coping in parents of children awaiting elective cardiac surgery. CTY. 2000; 10(03). 33. Wallander J. Theory-Driven Research in Pediatric Psychology: A Little Bit on Why and How. J Pediatr Psychol. 1992; 17(5): 521-535. congenital heart defects: A comprehensive review of literature. Journal of Social Service Research. 2012; 38(4), 484-502. 30. Swallow V, Lambert H, Santacroce S, Macfadyen A. Fathers and mothers developing skills in managing children’s long-term medical conditions: how do their qualitative accounts compare?. Child: Care, Health and Development. 2011; 37(4): 512-523. 31. Thompson R, Gustafson K, Hamlett K, Spock A. Stress, Rev. cienc. salud med. Volumen 3, Número 2, Mayo de 2016. 42