PAPEL DEL RECEPTOR DE FOLATO EN EL
CANCER DE OVARIO PLATINO-RESISTENTE
Andrés Poveda, MD
Ignacio Romero, MD
Area Clínica de Oncología Ginecologica
FUNDACION INSTITUTO VALENCIANO DE ONCOLOGIA
[email protected]
4th Ovarian Cancer Consensus Conference
June 25 – 27, 2010
UBC Life Sciences Institute, Vancouver, BC
B-2 What are the promising targets for future therapeutic approaches?
• The most promising targets in clinical trials are angiogenesis and homologous
recombination deficiency.
• To select patients for trials investigating these targets, predictive biomarkers are
required. Understanding mechanisms of resistance is a priority.
• Other promising targets currently being studied based on ovarian cancer biology
include:
• PI3-Kinase and Ras/Raf pathways
• Folate receptor
• Immune targets/cytokines, Notch/hedgehog, IGF merit further investigation.
• Targeted agents should be studied both as single agents and in combination based
on appropriate preclinical data.
Origen del folato en humanos
FOLATO= vitamina B9
ÁCIDO FÓLICO
pteroylmonoglutamic acid
ALIMENTACIÓN= FUENTE EXTERNA
60% legumbres + cereales
British Journal of Nutrition(2001), 85, Suppl. 2,
ENFERMEDADES ASOCIADAS DÉFICIT FOLATO
1) Anemia megaloblástica
2) Malformaciones recién nacido: maduración tubo neural
3) Homocisteinemia (¿?)
1) Acumulación de homocisteina
2) Efectos: factor riesgo cardiovascular: infartos,….
British Journal of Nutrition(2001), 85, Suppl. 2,
Folato: Claves
Se ingiere (nutrición)
Básico en la Síntesis de DNA
Parece pueda tener una relación con el
tratamiento del cáncer
Mecanismos de introducción FOLATO
en la célula
Substrato
Afinidad
Localización
tisular
Mcs
Dirección
Reduced Folate carrier
5-methyltetrahydrofolate
Baja
todos
iónico
bidireccional
FRA
FOLATO
Alta
Neoplasia
epitelial
(no requerido
en
condiciones
normales)
Endocitosis
Internalización
5-MTH: folato reducido (forma fisiológica mayoritaria)
esencial para la metilación génica (asociado a metilación de oncogenes): putativo papel protector en
carcinogénesis
RFC introduce los fármacos antifolato (MTX, Pemeterexed)
posible papel protector en CO (ver estudios supervivencia)
Kelemen Int. J. Cancer:119,243–250 (2006)
Zhao Expert Opin. Drug Deliv. (2008) 5(3):309-319
Folates can principally be taken up by 2 distinct mechanisms:
FR and RFC
The reduced folate carrier
binds folates with a low affinity
(Kd=10-5 M). Folic acid is a very
poor substrate.
Upon binding to the FR
(Kd=10-10 M), folic acid is
internalized via
endocytosis
2
1
Most antifolates enter
cells this way
Folic acid binds
to the FR with
high affinity
3
FR releases folic acid
inside the acidic
endosome
4
Folic acid escapes
endosome and enters
cytosol
5
FR recycles
back to cell surface
Mecanismo de acción del RF:
Endocitosis sin lisosomas
Folate-SMDCs enter cells via the FR
2
Upon binding to the folate receptor (Kd=1010 M), the conjugate is internalized via
endocytosis
The reduced folate carrier
Binds folates with a low affinity
(Kd=10-5 M). Folate conjugates
will not enter cell through the
reduced folate carrier.
most antifolates enter
cells this way
1
Folate-conjugate
binds the folate receptor
3
The drug is
cleaved inside
endosome
4
Drug escapes endosome
and exerts activity on
cell
5
Folate receptor recycles
back to cell surface
Mecanismos de introducción FOLATO
en la célula
Substrato
Afinidad
Localización
tisular
Mcs
Dirección
Reduced Folate carrier
5-methyltetrahydrofolate
Baja
todos
iónico
bidireccional
FRA
FOLATO
Alta
Neoplasia
epitelial
(no requerido
en
condiciones
normales)
Endocitosis
Internalización
5-MTH: folato reducido (forma fisiológica mayoritaria)
esencial para la metilación génica (asociado a metilación de oncogenes): putativo papel protector en
carcinogénesis
RFC introduce los fármacos antifolato (MTX, Pemeterexed)
posible papel protector en CO (ver estudios supervivencia)
Kelemen Int. J. Cancer:119,243–250 (2006)
Zhao Expert Opin. Drug Deliv. (2008) 5(3):309-319
La familia de RECEPTORES FOLATO α,β,γ
Macrófagos
asociados a
tumor
Forma
modificada:
mayor
afinidad
Folato
Antony AC. Folate receptors. Ann Rev Nutr 1996;16:501–21.
1. Low. Current Opin Chem Biol. 2009; 13:256-262
Pa
e
ti c
in
ea
l
ar
ta
ul
cr
cr
do
m
En
ic
ec
ic
st
tr
ea
ar
or
st
ol
G
Br
k
ey
ng
ec
dn
/N
Ki
e
n
NS
Lu
C
in
ri a
er
n/
ad
ai
Te
C
He
Br
va
Ut
O
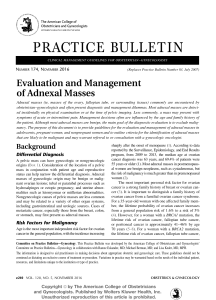
% FR Expression by IHC
Expresión de RFA en cáncer
100
90
80
70
60
50
40
30
20
10
0
Receptor Folato y Cáncer
• Expresión en Cáncer de Ovario
– Diana en Cáncer de Ovario
• Uso como Marcador pronóstico y predictivo de
eficacia
– Selección de pacientes: Imagen
• Aplicación clínica en Cáncer de Ovario
– Datos de estudios clínicos: PRECEDENT, PROCEED
• Aplicación clínica en otros tumores
RFA: Expresión en Cancer de Ovario (IHQ)
PRIMARY TUMOUR (72%, infraest)
PRIMARY vs RELAPSED (81%)
Agreement: 87.3%
Resumen: por qué RFA es una diana
interesante
1) LOCALIZACIÓN TEJIDO TUMORAL (no en sano)
2) ADQUIRIDO CON LA AGRESIVIDAD cáncer ovario
ESTADÍOS AVANZADOS
ALTO GRADO
3) Modelos in vitro/ in vivo inhibición inhibe crecimiento
4) MECANISMO ENDOCITOSIS PRESERVA MOLÉCULA
ASOCIADA
4th Ovarian Cancer Consensus Conference
June 25 – 27, 2010
UBC Life Sciences Institute, Vancouver, BC
B-2 What are the promising targets for future therapeutic approaches?
• The most promising targets in clinical trials are angiogenesis and homologous
recombination deficiency.
• To select patients for trials investigating these targets, predictive biomarkers are
required. Understanding mechanisms of resistance is a priority.
• Other promising targets currently being studied based on ovarian cancer biology
include:
• PI3-Kinase and Ras/Raf pathways
• Folate receptor
• Immune targets/cytokines, Notch/hedgehog, IGF merit further investigation.
• Targeted agents should be studied both as single agents and in combination based
on appropriate preclinical data.
Receptor Folato y CAO
• Papel del Receptor de Folato
– Diana potencial en Cáncer
• Expresión en Cáncer de Ovario
– Diana en Cáncer de Ovario
• Uso como Marcador pronóstico y predictivo de eficacia
– Selección de pacientes: Imagen
• Aplicación clínica
– Datos de estudios clínicos: PRECEDENT, PROCEED
Técnicas de imagen mediadas por receptor
Etarfolatide
• Requirimientos para un agente para imagen nuclear
– Alta afinidad para el receptor receptor1:
RA de Etarfolatide para FR: 0.92 (acido fólico: 1.0)2
– Selectividad alta:
FR sobreexpresado en cáncer1
– Aclaramiento rápido en tejido sano1:
t1/2= 25 minutos2
– Buena absorción para contraste1:
Etarfolatide molecular weight: 746 kD2
– Estabilidad
– Util para diagnóstico y cirugía3
SPECT/ Fluorescencia
1. Sega Cancer and Metastasis Reviews 2008 27 (4) 655-664;
2. Muller. Current Pharmaceutical Design, 2012, 18(8):1058-1082
3. Current Medicinal Chemistry, 2012, 19, 4742-4758
Etarfolatide: Características
CO2H
H2N
N
HN
O
N
N
H
N
O
O
H
N
O
O
H
N
N O
N
CO2H
Tc
NH2
S
CO2H
•Folate-targeted molecular imaging agent
•Companion diagnostic to vintafolide
•Minimally invasive technique to identify lesions that express folate
receptors
•Injected into subjects chelated with technetium 99m
•Detected by SPECT imaging (single-photon emission computerized
tomography)
1. Fisher. J Nucl Med 2008;49:899-906
Etarfolatide: distribución
Marrow
Liver
Kidney
Marro
w
Spleen
Bladder
FR positive lesions
Planar 99mTc-etarfolitide scan
Anterior
Posterior
Utilidad de Ac. Fólico para la calidad de imagen
Utilidad de Ac. Fólico para la calidad de imagen
Ovarian Cancer
Patient 1
Ovarian Cancer
Patient 1
Target
Lesion
No FA pre-injection
0.5 mg IV FA pre-injection
Correlación entre TAC y SPECT
Inguinal lymph node (1.5 cm- short axis)
FR-negative Lesion
Conjugados: Aplicación clínica
Etarfolatide
Cortesía Dr. I. Romero
Receptor Folato y Cáncer
• Papel del Receptor de Folato
– Diana potencial en Cáncer
• Expresión en Cáncer de Ovario
– Diana en Cáncer de Ovario
• Uso como Marcador pronóstico y predictivo de eficacia
– Selección de pacientes: Imagen
• Aplicación clínica
– Datos de estudios clínicos completados:
• EC-FV-02 y EC-FV-04 (PRECEDENT)
– Estudios clinicos en marcha: PROCEED
Aplicación clínica: Conjugados
Vintafolide (MK-8109, EC-145)
• A small drug conjugate of folate coupled chemically to
desacetylvinblastine hydrazide (DAVLBH) that specifically
targets the folate receptor (FR).
Vlahov, Bioconjugate Chem. 2012; 23(7)1357-1369
Leamon. Int J Cancer 2007; 121:1585-1592
Farletuzumab
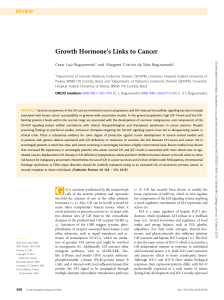
Current therapeutic approaches in
oncology
Leamon et al. (2013) Pharmacogenomics and Personalized Medicine 6, 113-125.
Tissue Distribution of Etarfolatide and Vintafolide in M109
Tumor-bearing Mice
3H-Vintafolide
or
Tu
m
om
St
M
us
cl
ac
h
e
y
id
ne
K
st
in
e
n
In
te
le
e
Sp
ve
r
Li
Lu
ng
ea
r
H
B
t
10
9
8
7
6
5
4
3
2
1
0
lo
od
% Injected Dose/Tissue (g)
Etarfolatide
1. Leamon. Proceedings of the 102nd Annual Meeting of the American Association for Cancer Research; AACR 2012. Abstract nr 3622.
Phase I Study of Folate Conjugate Vintafolide in
Patients with Refractory Solid Tumors
• MTD = 2.5 mg days 1, 3, and 5 and days 15, 17, and
19 of each 28-day cycle.
• One ovarian cancer patient with a RECIST-defined
partial response (PR) for a period of 111 days.
• One ovarian cancer patient with SD for 172 days.
• The most commonly reported adverse events were
constipation, nausea, fatigue, and vomiting.
Constipation was the dose-limiting toxicity.
FR status
EC20 status was determined from Etarfolatide imaging:
– EC20 (100%)
• all target lesions EC20 positive (subject score, 100%).
– EC20 (10-90%)
• at least one EC20-positive lesion but not all target lesions EC20
positive (subject score, 10%-90%).
– EC20(0%)
• no EC20-positive target lesions with at least one evaluable target
lesion (subject score, 0%)
– EC20 (?)
• no evaluable target lesions (subject score, nonevaluable).
Vintafolide in Subjects with Advanced Ovarian
Cancer: a Phase II study. Protocol EC-FV-02
Inclusion criteria
• Folate receptor (FR) positive platinum resistant or platinum
refractory epithelial ovarian, fallopian tube, or primary
peritoneal carcinoma
• Measurable disease with ≥ 1 target lesion by RECIST 1.0
• ≥ 4 prior chemotherapy regimen
• ECOG performance status 0-2
Exclusion criteria
• Pregnancy or lactating
• Symptomatic central nervous system metastasis
• Prior therapy with vinorelbine or other vinca-containing
compounds
Progression-Free Survival
Probability of Progression – Free Survival
1.0
Vintafolide ITT
(n=43)
Vintafolide ITT≤3
(n=15)
0.9
Progression, n
31
11
0.8
Censored, n
12
4
Median PFS
7.4
15.6
0.7
0.6
•
0.5
64% had 4 previous therapies
0.4
0.3
Vintafolide ITT
Vintafolide ITT≤3
0.2
0.1
0.0
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
Weeks From First Administration of Vintafolide
Vintafolide ITT ≤ 3 analysis set = patients in the trial who received three or fewer previous chemotherapy regimen
Results: Patients with ≤3 prior therapies
FR 100%
(N=7)
n (%)
FR 10-90%
(N=6)
n (%)
FR 0%
(N=1)
n (%)
FR NE
(N=1)
n (%)
Clinical Benefit
1 (14.3)
1 (16.7)
0 (0.0)
0 (0.0)
Response
Complete Response (CR)
Partial Response (PR)
Stable Disease (SD)
Progressive Disease (PD)
0 (0)
1 (14.3)
5 (71.4)
1 (14.3)
0 (0)
1 (16.7)
2 (33.3)
3 (50)
0 (0)
0 (0)
0 (0)
1 (100)
0 (0)
0 (0)
0 (0)
1 (100)
Overall Response (CR+PR)
1 (7.1)
1 (16.6)
0 (0)
0 (0)
Disease Control Rate
(CR+PR+SD)
6 (85.7)
3 (50)
0 (0)
0 (0)
PRECEDENT
n= 149 patients
Platinum resistant ovarian
cancer patients (failed first
or second platinum
therapy < 6 months)
EC20 Scan
2:1 Randomization
PRECEDENT: Randomized phase II Study of
PLD +/- Vintafolide in PROC
Vintafolide + PLD
Vintafolide 2.5mg TIW wks 1, 3
PLD=50 mg/m2 (IBW) every 28 days
PLD only
PLD= 50 mg/m2 (IBW) every 28 days
Statistical Analysis:
• Designed for 70% power for 0.68 HR for PFS analysis
• Stratification by region, line of platinum failure, baseline CA-125
• One pre-specified formal interim efficacy analysis for futility (DSMB)
• No protocol modifications following interim analysis
Key Inclusion/Exclusion Criteria
Inclusion criteria
Exclusion criteria
• Pathology-confirmed platinum• Borderline tumors
resistant ovarian cancer
• Prior exposure to PLD, folate receptor• ≥ 1 RECIST-defined measurable lesion
targeted therapy, mouse antibodies,
(RECIST 1.0—up to 10 lesions)
vinorelbine or other vinca-containing
• Prior platinum-based chemotherapy
compounds
but ≤ 2 prior systemic cytotoxic
• Other concurrent chemotherapy,
regimens (allowed 1 prior line of nonimmunotherapy, radiotherapy, or any
cytotoxic therapy)
other investigational therapy.
• ECOG performance status of 0 to 2
with adequate organ function
Primary endpoints
Efficacy
• Progression-free survival (PFS)
Safety
Secondary efficacy endpoints
• Overall survival (OS)
• Correlation between therapeutic
response and folate receptor (FR)
positivity in the following subgroups:
–FR (100%)
–FR (10-90%)
–FR (0%)
Etarfolatide: Subgroup assignment for PRECEDENT
Subgroup
FR(100%)
FR
expression
% PRECEDENT
Population
All target
lesions
40.4%
At least one target lesion 78.7%
FR (10-90%)
FR(-)
At least one,
but not all
target lesions
38.3%
No target
lesions
21.3%
Primary Endpoint: Progression Free Survival (PFS)
Stratification
Progression-Free Survival: Subgroup Analysis
Vintafolide +
PLD
PLD Alone
HR
p-value
n
PFS
(mos)
n
PFS
(mos)
(95% CI)
Logrank
ITT
100
5.0
49
2.7
0.626
(0.409, 0.959)
0.031
FR (10 -100%)
48
5.7
26
1.7
0.547
(0.304, 0.983)
0.041
FR (100%)
23
5.5
15
1.5
0.381
(0.172, 0.845)
0.013
FR (10-90)
25
5.7
11
7.0
0.873
(0.334, 2.277)
0.791
13
3.8
7
5.4
1.806
(0.369, 8.833)
0.468
Population
FR (0%)
Progression-Free Survival
Subgroup Analyses – FR(100%)
Variable
Median PFS (wk)
Hazard Ratio
p-value (2-sided Test)
Vintafolide +
PLD Alone
PLD
24.0
6.6
0.387
0.013
Progression-Free Survival
Subgroup Analyses FR (0%)
Variable
Median PFS (wk)
Hazard Ratio
p-value (2-sided Test)
Vintafolide
+ PLD
PLD
Alone
16.6
23.3
1.806
0.468
Drug-Related Adverse Reaction Occurring in ≥10% of
Patients in Either Treatment
Conclusions
• Platinum resistant ovarian cancer (PROC) is an orphan indication with high
unmet medical need.
• The results of PRECEDENT demonstrate statistically significant and clinically
meaningful improvement in progression-free survival (PFS) for patients with
PROC, with the greatest efficacy in patients where all target lesions where FR
positive (FR 100%)
•
Estudio PROCEED
Overall, the safety data suggest that,
with appropriate
monitoring, vintafolide +
FASE
III
PLD is well tolerated by subjects regardless of their FR status
• Vintafolide + PLD demonstrated an overall positive risk-benefit assessment
• Improved risk-benefit profile for the FR(100%) subject population
• FR(0%) subjects should not be treated with the combination regimen
• These results support the use of etarfolatide to identify PROC patients with FR
positive disease.
20 March 2014
EMA/CHMP/138539/2014
Committee for Medicinal Products for Human Use (CHMP)
Su m m a r y of opin ion 1 ( init ia l a u t hor isa t ion)
Vynfinit
vintafolide
On 20 March 2014, the Committee for Medicinal Products for Human Use (CHMP) adopted a positive
opinion, recommending the granting of a conditional marketing authorisation 2 for the medicinal
product Vynfinit, intended for the treatment of adult patients with platinum-resistant ovarian cancer
who express the folate receptor on all target lesions. Folate receptor status should be assessed by a
diagnostic medicinal product approved for the selection of adult patients for treatment with vintafolide,
such as Folcepri (see Summary of Opinion on Folcepri).
Vynfinit was designated an orphan medicinal product on 9 February 2012. The applicant for this
medicinal product is Endocyte Europe, B.V.
Vynfinit is to be available as a 2.5 mg powder for solution for injection. The active substance of Vynfinit
is vintafolide, which belongs to the therapeutic group ‘vinca alkaloid and analogues’ (L01CA06).
Vintafolide consists of folic acid and the cytotoxic agent desacetylvinblastine hydrazide (DAVLBH). The
folic acid component enables DAVLBH to be delivered preferentially to cancer cells expressing folate
receptors. Once delivered inside cancer cells, DAVLBH is released from vintafolide and acts by
inhibiting microtubule assembly and arresting cells in mitosis.
The benefits with Vynfinit are its ability, in combination with pegylated liposomal doxorubicin (PLD), to
improve progression-free survival in patients with platinum-resistant ovarian cancer when compared
with treatment with PLD alone. The most common side effects are fatigue, stomatitis, neutropenia,
anaemia, nausea, palmar-plantar erythrodysaesthesia, constipation, rash and peripheral sensory
neuropathy.
A pharmacovigilance plan for Vynfinit will be implemented as part of the marketing authorisation.
The text for the approved indication is as follows: "Vynfinit in combination with pegylated liposomal
doxorubicin (PLD) is indicated for the treatment of adult patients with platinum resistant ovarian
PROCEED: Phase 3 Study EC-FV-06:
PLD +/- Vintafolide in PROC Patients
N= 640 patients
Platinum resistant ovarian cancer
patients (failed first or second
platinum therapy < 6 months)
Up to 2 prior lines
Vintafolide + PLD
Receptor Scan
1:1
Vintafolide= 2.5mg TIW wks 1, 3
PLD=50 mg/m2 (IBW) every 28 days
PLD + placebo
50 mg/m2 (IBW) every 28 days
Same Design
as Phase 2
Increased Probability
for Success
Robust Assessment of PFS (and
OS)
Clinically Meaningful PFS
Improvement
•Platinum resistant ovarian cancer
•Same dose and schedule
•Exclude FR(0%) patients from study
•Increase power for OS (85% power for HR= 0.70)
•Double-blinded
•Radiologic progression only, RECIST v1.1
•Supportive blinded independent review
•Primary endpoint on FR 100%
•Final PFS analysis = 98% power for HR= 0.60
•Step-down analysis for low FR thresholds
Conclusiones
• Los receptores folato están sobreexpresados en la mayor parte de los tumores
epiteliales. Su sobreexpresión está asociada a un peor pronóstico.
• Los RF pueden ser utilizados para transportar al interior de la célula moléculas
para uso diagnóstico y terapéutico.
• Etarfolatide (conjugado Ac. Fólico con Tc99) ha demostrado alta afinidad para
unirse a RF y detectar tumores RF(+) mediante SPECT.
• Datos de Fase-II randomizado de Vintafolide (conjugado de Ac. Fólico con una
Vinca), en combinación con PLD vs PLD ha demostrado eficacia en el tratamiento
del cáncer de ovario platino-resistente.
• La eficacia de Vintafolide va asociada a los tumores con mayor porcentaje de
RF(+), definido por técnicas de imagen (Etarfolatide - SPECT).
• Estudio PROCEED (F III) en cáncer de ovario recurrente, en población resistente,
en fase de reclutamiento activo.
Let´s go…
[email protected]
 0
0