diagnóstico diferencial y manejo de la ascitis
Anuncio

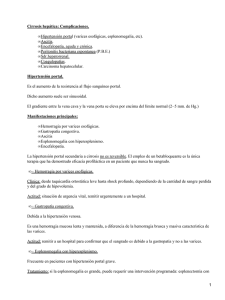
t In a in ic E ed L M U o CA ci i rv Se DIAGNÓSTICO DIFERENCIAL Y MANEJO DE LA ASCITIS SESIONES BIBLIOGR ÁFICAS RESIDENTES na er MARI CRUZ PÉREZ PANIZO MIR MEDICINA INTERNA COMPLEJO ASISTENCIAL UNIVERSITÁRIO DE LEÓN 11-6-2012 DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Causas na er t In a in ic E ed L M U o CA ci i rv Se -Obesidad abdominal- distinguir ascitis de grasa: tiempo de evolución -Cirrosis: causa más frecuente de ascitis -Hepatitis alcohólica con o sin cirrosis -Hepatitis viral C: transfusiones antes de 1990, compartir agujas, tatuajes, acunpuntura,emigración A Japón ó sudeste asiático -Hepatitis B: tranfusion antes de 1971, áreas hiperendemicas (África, Sudeste asiático:China, Corea, Indonesi y Filipinas, oriente medio excepto Israel, islas del pacifico sur y oeste, cuenca interior del Amazonas y partes del Caribe: Haití y R.Dominicana), varones homosexuales, UDVP, Dialisis, VIH y contactos. -Historia familiar de enfermedad hepática: Hemocromatosis, Wilson -Esteatohepatitis no alcohólica: antes criptogenética: obesidad, DM, DL: riesgo de “ “ “ según nº de años con IMC>30Kg/m2 -Complicación de una cirrosis compensada: por daño hepático viral o hepático sobre la previa cirrosis, desarrollo de hepatocarcinoma -si no cumple anamnesis ni caracteristicas clinicas ni pruebas complementarias de cirrosis: otras causas: cancer, ICC, TBC, Hemodialisis (ascitis nefrogénica) y pancreatitis. CAUSES OF ASCITES Heart failure Tuberculosis 10 percent 3 percent 2 percent 1 percent na er Dialysis 81 percent t In a in ic E ed L M U o CA Cancer ci i rv Se Cirrhosis Pancreatic disease 1 percent Other 2 percent Data from: Runyon, BA, Hoefs, JC, Morgan, TR. Ascitic fluid analysis in malignancy‐related ascites. Hepatology 1998; 8:1104. Causes of malignancy‐related ascites Peritoneal carcinomatosis t In a in ic E ed L M U o CA ci i rv Se Cause Frequency among patients with malignancy­related ascites Massive liver metastases causing portal hypertension 53 percent 13 percent Hepatocellular carcinoma plus cirrhosis 13 percent Chylous ascites due to malignancy, usually lymphoma 7 percent Budd‐Chiari syndrome due to malignancy occluding the hepatic veins Rare na er Peritoneal carcinomatosis plus massive liver 13 percent metastases Rare causes of ascites Infectious Miscellaneous Amyloidosis Abdominal pregnancy Castleman's syndrome Crohn's disease i rv Extramedullary hematopoiesis Chlamydia peritonitis Hemophagocytic syndrome Histiocytosis X Leukemia Complications related to HIV infection Lymphoma Pelvic inflammatory disease Multiple myeloma Gaucher's disease Lymphangioleiomyomatosis Myxedema Nephrotic syndrome (in children, adults with nephrotic syndrome and ascites usually have another cause such as cirrhosis) Operative lymphatic tear or ureteral injury na Pseudomembranous colitis Endometriosis er Salmonellosis Mastocytosis t In a in ic E ed L M U o CA Brucellosis ci Ascariasis Rare causes of ascites Hematologic Se Amebiasis Rare causes of ascites Ovarian hyperstimulation syndrome POEMS syndrome Whipple's disease Systemic lupus erythematosus Ventriculoperitoneal shunt i rv Se CAUSA MÁS FRECUENTE DE ASCITIS: CIRROSIS HEPÁTICA: na er t In a in ic E ed L M U o CA ci 1.COMPLICACIONES POR LA HTPORTAL: -HDA POR VARICES ESOFÁGICAS O POR GASTROPATÍA DE LA HTP -ASCITIS: ES LA COMPLICACIÓN MÁS FRECUENTE -EPH 2.COMPLICACIONES POR LA ASCITIS: -PBE -SÍNDROME HEPATORRENAL i rv Se ASCITIS DEBIDA A MÁS DE UNA CAUSA: 5% de pacientes aprox. Diagnóstico más confuso: cada causa por separado no es tan severa como para provocar la cuantía ascítica observada t In a in ic E ed L M U o CA ci Las más frecuentes que coexisten: Cirrosis + peritonitis TBC “ + carcinomatosis peritoneal “ + ICC “ + nefropatía diabética Complicaciones obesidad: nefropatia diabética + ICC + cirrosis debida a Esteatohepatitis no alcohólica na er DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Exploración física na er t In a in ic E ed L M U o CA ci i rv Se Estigmas de cirrosis: excepción el paciente de pigmentación oscura (no son aparentes ni las arañas vasculares ni el eritema palmar), colaterales abdominales de extensión cefálica, son raras las arañas vasculares por debajo del ombligo. Ictericia Pérdida de masa muscular Leuconiquia: uñas de Muehrcke, Terry Hipertrofia parotídea bilateral (por alcohol y no por la cirrosis en si) Hepatoesplenomegalias palpables (puede) Palpación hepática: blando, grande y firme más en hepatitis enólica que en hepatocarcinoma Principal: matidez en flancos que además se cambia al rotar al paciente Si ↑PVY orienta a ICC ó Pericarditis constrictiva como causa de ascitis ( o al menos una de las causas) DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Exploración física na er t In a in ic E ed L M U o CA ci i rv Se Pacientes alcohólicos con miocardiopatia dilatada enólica y ascitis, se les infradiagnostica frecuentemente la ICC: en eco se ve ascitis y se etiqueta de cirrosis sin estar presente: importante distinción por distintas implicaciones terapéuticas. Nódulo (umbilical) de la hermana MªJosé: cáncer como causa de la ascitis: gástrico, cólon, hepatocelular, linfoma (AP da Dx) DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Diagnóstico na er t In a in ic E ed L M U o CA ci i rv Se Exploración fisica: S:50-94% y E: 29-82% comparados con el gold standard: eco abdominal Tres grados de ascitis: 1 LEVE(solo detectable por eco), 2 MODERADA (distensión simétrica mod abd) y 3 SEVERA (marcada distensión abd): 1+ a 4+(masiva y a tensión) Matidez en flancos: 1500ml Eco abdominal: 100-150ml detecta. Ver higado y bazo: si ≥12 cm ó recanalizacion v.umbilical →evidencia indirecta de HTP. Detecta obstrucc biliar, hepatocarcinoma Paracentesis: confirma ascitis, dx etiologia y dx si hay infección Indications for abdominal paracentesis in a patient with ascites New onset ascites At the time of each admission to the hospital Fever Mental status change Ileus Hypotension Laboratory abnormalities that may indicate infection Acidosis Worsening of renal function Gastrointestinal bleeding (a high risk time for infection) na Peripheral leukocytosis er t In a in ic E ed L M U o CA Abdominal tenderness ci Abdominal pain i rv Se Clinical deterioration, either inpatient or outpatient DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Paracentesis Diagnóstica Se Apariencia, transparencia, turbidez, lechoso (ascitis quilosa: causa na er t In a in ic E ed L M U o CA ci i rv + frec: neo/cirrosis/traumatismo linfaticos) rosado(>10000 eritrocitos/mm3), rojo (>>10000 eritrocitos/mm3) Iniciar atb empirico si neutrofilos ≥250/mm3 Sangrado traumatico: heterogeneo, no traumatico es homogéneo Ascitis hemorrágica: fuga por pinchazo de colateral, cirrosis, cancer(hepatocarcinoma pueden desarrollar un sangrado masivo intraabdominal) TBC peritoneal raramente es hemorragica Ascitis marron: y Bilirrubina es mayor q la sérica: ulcera duodenal perforada o rotura vesicula DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Líquido ascítico Se t In a in ic E ed L M U o CA ci i rv Esta infectado? Nº células Hay HTP? Gradiente Albúmina sérica-Albúmina ascítica na er El nº de células en liquido ascítico nos hará tomar decisiones de vida o muerte por ello es imprescindible tener el resultado cuanto antes: si el liquido esta infectado y no ponemos atb el paciente puede fallecer DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Líquido ascítico Se t In a in ic E ed L M U o CA ci i rv Esta infectado? Nº células Hay HTP? Gradiente Albúmina sérica-Albúmina ascítica na er En ICC y ascitis el gradiente As-Aa puede estrecharse pero en cirrosis permanece estable a no ser que baje la TA mucho DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Líquido ascítico Se t In a in ic E ed L M U o CA ci i rv Esta infectado? Nº células Hay HTP? Gradiente Albúmina sérica-Albúmina ascítica na er ¿Cultivos? Si en ascitis de inicio, deterioro (fiebre, dolor abdominal, azoemia, acidosis o confusion) no necesario en paracentesis terapéuticas y sin síntomas/signos de infección ¿Cómo? 10ml de liquido ascítico mejor en frascos de hemocultivos DIAGNÓSTICO DIFERENCIAL DE LA ASCITIS Líquido ascítico Se t In a in ic E ed L M U o CA ci i rv Esta infectado? Nº células Hay HTP? Gradiente Albúmina sérica-Albúmina ascítica na er Proteinas totales<1 g/dL: alto riesgo de PBE: dar atb selectivos para prevenir Glucosa baja por consumo de bacterias y tb en carcinomatosis peritoneal, indetectable en perforacion intestinal al l.ascitico na er t In a in ic E ed L M U o CA ci i rv Se ≥1.1 GRADIENTE As-Aa : HTP <250 PMN <500 <2,5g/dL PT en L.A. ≥2,5g/dL PT en L.A. <1.1 GRADIENTE As-Aa: no HTP Se <2,5g/dL PT en L.A. ≥250 PMN ≥1.1 GRADIENTE As-Aa : HTP t In a in ic E ed L M U o CA LEUCOCITOS LIQUIDO ASCITICO ci i rv ≥50% PMN <1.1 GRADIENTE As-Aa: no HTP ≥1.1 GRADIENTE As-Aa : HTP na er <50%PMN ≥500 <1.1 GRADIENTE As-Aa: no HTP cultivo + 1 microorg <1g/dLPT Gluc>50mg/dL, LDH<225 Polimicrob, PT>1g/dL, Gluc<50, LDH≥225 Amilasa L.A.>100 Citologia + Enviar cultivo micobacterias Citologia + Enviar cultivo micobacterias na er t In a in ic E ed L M U o CA ci i rv Se Ascitis cirrótica no complicada Ascitis cardiaca Ascitis nefrótica Peritonitis bacteriana espontanea Peritonitis bacteriana secundaria Ascitis pancreática Carcinomatosis peritoneal con HTP Peritonitis TBC con cirrosis de base Carcinomatosis peritoneal Peritonitis TBC na er t In a in ic E ed L M U o CA ci i rv Se Eco abdominal y/o bx hepática Rx tórax y ecocardiograma Proteinuria de 24h Respuesta clínica a antibióticos Estudios contraste hidrosoluble intestinal(enema opaco) TAC abdominal Búsqueda de tumor primario Bx peritoneal laparoscopica y cultivo micobacterias Cirugia si se documenta perforacion intestinal tuberculostaticos American Association for the Study of Liver Diseases (AASLD) recommendations for the management of adult patients with ascites due to cirrhosis i rv Se 1.Evaluation and diagnosis t In a in ic E ed L M U o CA ci Abdominal paracentesis should be performed and ascitic fluid should be obtained from inpatients and outpatients with clinically apparent new‐onset ascites. Because bleeding is sufficiently uncommon, the routine prophylactic use of fresh frozen plasma or platelets before paracentesis is not recommended. na er Data from: Runyon BA. Management of adult patients with ascites due to cirrhosis: an update. Hepatology 2009; 49:2087. 2.Differential diagnosis t In a in ic E ed L M U o CA ci i rv Se The initial laboratory investigation of ascitic fluid should include an ascitic fluid cell count and differential, ascitic fluid total protein, and serum‐ascites albumin gradient (SAAG). If ascitic fluid infection is suspected, ascitic fluid should be cultured at the bedside in blood culture bottles prior to initiation of antibiotics. na er Other studies of ascitic fluid can be ordered based on pretest probability of disease. Testing serum for CA125 is not helpful in the differential diagnosis of ascites. Its use is not recommended in patients with ascites of any type. Optional tests Total protein concentration Culture in blood culture bottles Glucose concentration LDH concentration t In a in ic E ed L M U o CA Albumin concentration ci Cell count and differential i rv Se Routine tests Gram stain Amylase concentration Unusual tests Tuberculosis smear and culture na er Cytology Triglyceride concentration Bilirubin concentration 3.Treatment of ascites Patients with ascites who are thought to have an alcohol component to their liver injury should abstain from alcohol consumption. Se t In a in ic E ed L M U o CA ci i rv Firstline treatment of patients with cirrhosis and ascites consists of sodium restriction (88 mmol/day [2000 mg/day]) and diuretics (oral spironolactone with or without oral furosemide). Fluid restriction is not necessary unless serum sodium is less than 120 to 125 mmol/L. na er An initial therapeutic abdominal paracentesis should be performed in patients with tense ascites. Sodium restriction and oral diuretics should then be initiated. Diuretic‐sensitive patients should preferably be treated with sodium restriction and oral diuretics rather than with serial paracenteses. Liver transplantation should be considered in patients with cirrhosis and ascites. na er t In a in ic E ed L M U o CA ci i rv Se t In a in ic E ed L M U o CA ci i rv Se na er CT scan shows a large volume of ascitic fluid surrounding a small shrunken cirrhotic liver. The fluid is of low attenuation and is free floating without septations or solid material. Courtesy of Jonathan Kruskal, MD. Se 5.Hepatorenal syndrome t In a in ic E ed L M U o CA ci i rv Albumin infusion plus administration of vasoactive drugs such as octreotide and midodrine should be considered in the treatment of type I hepatorenal syndrome. na er Patients with cirrhosis, ascites, and type I hepatorenal syndrome should have an expedited referral for liver transplantation. 6.Spontaneous bacterial peritonitis (SBP) Se Patients with ascites admitted to the hospital should undergo abdominal paracentesis. Paracentesis should be repeated in patients (whether in the hospital or not) who develop signs or symptoms or laboratory abnormalities suggestive of infection (eg, abdominal pain or tenderness, fever, encephalopathy, renal failure, acidosis, or peripheral leukocytosis). t In a in ic E ed L M U o CA ci i rv Patients with ascitic fluid PMN counts ≥250 cells/mm3 (0.25 X 109 /L) should receive empiric antibiotic therapy, eg, an intravenous third‐generation cephalosporin, preferably cefotaxime 2 g every 8 hours. Oral ofloxacin (400 mg twice per day) can be considered a substitute for intravenous cefotaxime in inpatients without prior exposure to quinolones, vomiting, shock, grade II (or higher) hepatic encephalopathy, or serum creatinine >3 mg/dL. na er Patients with ascitic fluid polymorphonuclear leukocyte (PMN) counts <250 cells/mm3 (0.25 X 109 /L) and signs or symptoms of infection (temperature >100°F or abdominal pain or tenderness) should also receive empiric antibiotic therapy, eg, intravenous cefotaxime 2 g every 8 hours, while awaiting results of cultures. When the ascitic fluid of a patient with cirrhosis is found to have a PMN count ≥250 cells/mm3 (0.25 X 109/L) and there is high suspicion of secondary peritonitis, it should also be tested for total protein, LDH, glucose, Gram stain, carcinoembryonic antigen, and alkaline phosphatase to assist with the distinction of SBP from secondary peritonitis. Patients with ascitic fluid PMN counts ≥250 cells/mm3 (0.25 X 109 /L) and clinical suspicion of SBP, who also have a serum creatinine >1 mg/dL, blood urea nitrogen >30 mg/dL, or total bilirubin >4 mg/dL should receive 1.5 g albumin/kg body weight within 6 hours of detection and 1.0 g/kg on day 3. 7.Prevention of spontaneous bacterial peritonitis Intravenous ceftriaxone for 7 days or twice‐daily norfloxacin for 7 days should be given to prevent bacterial infections in patients with cirrhosis and gastrointestinal hemorrhage. Se t In a in ic E ed L M U o CA ci i rv Patients who have survived an episode of SBP should receive long‐term prophylaxis with daily norfloxacin (or trimethoprim/sulfamethoxazole) because this is the most data‐supported indication for long‐term outpatient prophylaxis. na er In patients with cirrhosis and ascites but no gastrointestinal bleeding, long‐term use of norfloxacin (or trimethoprim/sulfamethasoxazole) can be justified if the ascitic fluid protein <1.5 g/dL and at least one of the following is present: serum creatinine ≥1.2 mg/dL, blood urea nitrogen ≥25 mg/dL, serum sodium ≤130 mEq/L, or Child‐Pugh ≥9 points with bilirubin ≥3 mg/dL. Intermittent dosing of antibiotics to prevent bacterial infections may be inferior to daily dosing (due to the development of bacterial resistance) and thus daily dosing should preferentially be used. na er t In a in ic E ed L M U o CA ci i rv Se BIBLIOGRAFÍA Se na er t In a in ic E ed L M U o CA ci i rv UpToDate: • Diagnosis and evaluation of patients with ascites, Bruce A Runyon, MD, Marshall M Kaplan, MDPeter A L Bonis, MD, last updated: nov 16, 2011. • Initial therapy of ascites in patients with cirrhosis, José Such, MD, PhD, Bruce A Runyon, MD, Marshall M Kaplan, MD, Peter A L Bonis, MD, last updated: abr 25, 2011 • Treatment of diuretic‐resistant ascites in patients with cirrhosis, José Such, MD, PhD Bruce A Runyon, MD Paul Angulo, MD Peter A L Bonis, MD, last updated: abr 27, 2012. • Malignancy‐related ascites, Bruce A Runyon, MD, Lawrence S Friedman, MD, Peter A L Bonis, MD, last updated: jun 9, 2010 • Chylous, bloody, and pancreatic ascites Andrés Cárdenas, MD, MMSc, AGAF, Andres Gelrud, MD, Sanjiv Chopra, MD, Bruce A Runyon, MD, Anne C Travis, MD, MSc, FACG, last updated: abr 17, 2012. BIBLIOGRAFÍA na er t In a in ic E ed L M U o CA ci i rv Se • Varios Autores. Manual CTO Medicina y Cirugía, 7ª Edición, Tomo I, 330‐337, y Adenda. • Harrison's principles of internal medicine, 18th Edition, Part , Section , Chapter : • Martín Asenjo, R., Bastante Valiente, M.T., Torres Macho, J. Manual de diagnóstico y Terapéutica Médica. H.U. 12 de Octubre, 6ª Edición, • Jiménez Murillo, L., Montero Pérez, F.J., Guía Terapéutica. Medicina de Urgencias, 3ª Edición, • De Castro Del Pozo, S. Manual de Patología General, 5ª Edición, VALORACIÓN FUNCIONAL DE LA CIRROSIS: CLASIFICACIÓN DE CHILD‐PUGH GRADO 1 GRADO 2 GRADO 3 EPH No 1 a 2 3 a 4 ASCITIS Ausente Ligera Moderada BILIRRUBINA(mg/dl) 1 a 2 2 a 3 >3 ALBÚMINA (g/l) >35 ACTIVIDAD DE PROTROMBINA >50% t In a in ic E ed L M U o CA ci i rv Se PARÁMETRO 28 a 35 <28 30‐50% <30% na er CHILD‐PUGH A (Leve) 5 ‐ 6 CIRUGÍA B 7 ‐ 9 TIPS C 10 ‐ 15 TIPS GRACIAS A TODOS na er t In a in ic E ed L M U o CA ci i rv Se