of Ocular Surface Squamous Neoplasia Herpes simples Ceratite pelo vírus
Anuncio

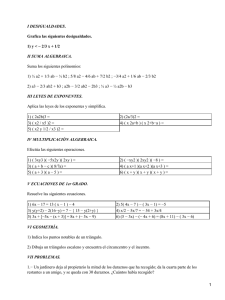
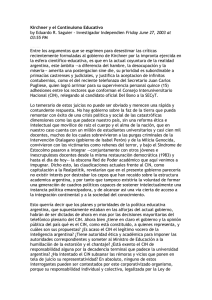
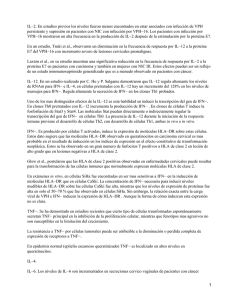
Volumen IV No.2 Junio 2005 Interferon Alfa 2b in the Medical Management of Ocular Surface Squamous Neoplasia Aaleya F. Koreishi, MD and Carol L. Karp, MD Ceratite pelo vírus Herpes simples Denise de Freitas, MD Aspectos Genéticos y Oftalmológicos del Síndrome de Axenfeld Rieger Rodolfo A. Pérez Grossmann, MD Junio 2005 MENSAJE DEL PRESIDENTE A todos los miembros de la Asociación Panamericana de Oftalmología: sumir la presidencia de la Asociación Panamericana de Oftalmología es probablemente el mayor honor al que pueda aspirar un oftalmólogo Latinoamericano. La APAO es una organización supranacional que incluye, sin excepción, a todos los países de este continente con tres lenguas oficiales y más de 15,000 miembros en ella. Es también, sin duda, de las organizaciones supranacionales existentes en el mundo la más activa e intensa. De hecho, en su género, es un modelo y aspiración de las otras entidades supranacionales que se integran dentro del Concilio Internacional de Oftalmología. Nuestra asociación se reúne en forma bianual y sin interrupciones desde hace más de 50 años. Acaba de concluir el XXV Congreso Panamericano celebrado en la Ciudad de Santiago, Chile. Más de 2,500 oftalmólogos estuvieron presentes. La organización fue perfecta gracias al esfuerzo que efectuó el Comité Organizador que encabezó brillantemente el Dr.Juan Verdaguer. Los trabajos del Congreso se desarrollaron en un ambiente académico, de interés y cordialidad. El Congreso de Santiago fue un placer para todos aquellos que tuvimos la oportunidad de asistir. Los Congresos Panamericanos son el Enrique Graue momento cúspide de nuestra AsociaPresidente de la Asociación Panamericana de Oftalmología. ción, en su organización empeñamos muchos esfuerzos y atención pues reflejan fielmente el estado de la Oftalmología de este continente y son la oportunidad que tenemos de presentarnos, aquilatarnos, conocernos y estrechar amistades. La actividad académica que en ellos se despliega es de tal intensidad que en Santiago estuvieron presentes más de 1200 oftalmólogos que activamente presentaron sus experiencias y compartieron conocimientos. Por ello, el próximo año en febrero del 2006, en Sao Paulo, en conjunción con el Congreso Mundial de Oftalmología, la APAO se reunirá a esta organización como parte integral del Congreso y tendremos en él, la oportunidad de exponer nuestra oftalmología ante el resto del mundo en un ambiente único, precarnaval, en la hermosa ciudad de Sao Paulo. Ese será el XXVI Congreso de nuestra asociación. Para el año 2007, en el mes de mayo, en Cancun, México, nos volveremos a reunir. Para el efecto ya se encuentra trabajando activamente el comité Organizador de lo que será el XXVII Congreso Panamericano. Para el año 2009 ya se han propuesto dos ciudades de nuestro continente; Cartagena en Colombia y Punta del Este en Uruguay. En ambos casos los comités nacionales se han comenzado a integrar y a elaborar sus propuestas para que en la asamblea de Directores en Chicago, en este año, se vote y defina la sede del XXVIII Congreso Panamericano de Oftalmología. Si bien los congresos son un componente muy importante de cualquier agrupación médica, en la APAO no lo son todo. Nuestra agrupación tiene una intensa actividad que abarca otras muchas ramas. Anualmente se organizan cursos regionales en donde se revisan con finalidades educativas temas de actualidad. Para el efecto este año nos reuniremos en Tucumán Argentina y en Chihuahua, México. Un Comité específico de nuestra asociación se encarga de estos cursos de corta duración. La Asociación esta también activa en las políticas regionales de prevención de ceguera; de promoción de bancos de ojos; en este boletín; en la comunicación electrónica en la página web; en la educación médica de nuestros residentes; en la organización de cursos básicos en oftalmología; en la génesis de políticas regionales de relaciones profesionales y A en la formación de jóvenes oftalmólogos que serán los líderes de nuestra profesión en el futuro; en el otorgamiento de becas para la superación académica y de investigación; en la Academia Americana de Oftalmología con cursos Preacademia y de resumen de lo mejor que se presenta en ella; en la formación de personal paramédico y en todas aquellas actividades que puedan ayudar a superar la oftalmología intercontinental o que puedan afectar su desarrollo. En todo ello esta presente la Asociación Panamericana de Oftalmología. Al asumir la Presidencia de la misma, asumo con ello el compromiso de continuar haciendo todo lo anterior, que es mucho y bueno. Empezaremos por poner un especial énfasis en la educación y estándares de las residencias en Latinoamérica, Para el efecto, este año, iniciaremos con un curso en combinación con Internacional Council of Ophthalmology y la Asociación de Profesores Universitarios de Oftalmología ( AUPO) de los Estados Unidos de Norteamérica encaminado a " Enseñar a enseñar " a aquellos encargados de las residencias de oftalmología de nuestro continente. Como siempre, nada de lo que se quiera hacer será posible sin la participación de todos nosotros, de ustedes como miembros titulares de nuestra asociación, de las mesas directivas de cada una de las sociedades nacionales, de sus representantes delegados a la Asamblea del Board of Directors y del propio Comité Ejecutivo la Asociación. Con la participación de todos conseguiremos una mejor Asociación Panamericana de Oftalmología. To all the members of the Pan-American Association of Ophthalmology: o assume the presidency of the Pan-American Association of Ophthalmology is probably the greatest honor to which a Latin American ophthalmologist can aspire. The PAAO is a supranational organization that includes, without exception, all the countries of this continent with three official languages and more than 1500 members. Moreover, it is without a doubt, the most active and intensive of all the supranational organizations in the world. As a result, it is a model for other supranational entities that belong to the International Council of Ophthalmology. Our association has met every two years without interruption for more than 50 years. At the recent 25th Pan-American Congress in Santiago, Chile, more than 2500 ophthalmologists were present. The organization was perfect as designed by the organizing committee led brilliantly by Dr. Juan Verdaguer. The activities of the Congress took place in an academic atmosphere one of interest and cordiality. The Congress in Santiago was a pleasure for all those who had the opportunity to participate. The Pan-American congresses are the apex of our association, in whose organization we invest great effort and attention, reflecting accurately the state of ophthalmology on this continent and gives the opportunity to present and test ideas, to make acquaintances and to extend friendships. The academic activity developed with such intensity that in Santiago there were more than 1200 ophthalmologists who presented their experiences and imparted their knowledge. Next year in February 2006, in Sao Paulo, in conjunction with the World Congress of Ophthalmology, PAAO will join as an integral part of that congress, and we will have the opportunity to export our ophthalmology to the entire world in an atmosphere of unity, just before carnival in the lovely city of Sao Paulo. This will be the 26th congress of our association. In May 2007 in Cancun, Mexico, we will meet once again. The organizing committee of the 27th Pan-American Congress is already at work. For 2009, two sites have been proposed: Cartagena in Colombia and Punta del Este in Uruguay. In both cases, the national committees have T VISIONPAN-AMERICA : 1 : Junio 2005 PRESIDENT’S MESSAGE UMA MENSAGEM DO PRESIDENTE begun to develop their proposals for the Executive Committee in Chicago this year, who will vote on the site of the 28th Pan-American Congress of Ophthalmology. Even though congresses are a very important component of any medical association, in the PAAO, they do not represent all that we have to offer. Our association is intensely active in a variety of areas. Annually, the PAAO organizes regional courses where the educational goals are practical themes. With this intent, we will meet this year in Tucuman, Argentina and in Chihuahua, Mexico. A special committee of our association designs these short courses. The Association is also active in regional politics for the prevention of blindness; in the promotion of eye banking; in this publication; in communication via our web page; in the medical education of our residents; in organizing basic courses in ophthalmology; in regional politics, professional relations, and in the development of young ophthalmologists who will be the leaders of our profession in the future; in supporting academic scholarships and research; in the American Academy of Ophthalmology with pre-Academy courses and the "Best of the AAO"; in the promotion of paramedical personnel in all the activities that can assist and help develop intercontinental ophthalmology. And in all these areas, the Pan-American Association of Ophthalmology is a presence. In assuming the presidency of the PAAO, I take on the responsibility to continue all that I have described. We are beginning to place emphasis on the education of residency directors in Latin America. To this end, this year in conjunction with the International Council of Ophthalmology (ICO) and the Association of University Professors of Ophthalmology (AUPO) from the United States, we will initiate a course called "Educating the Educator" for those responsible for ophthalmology residency programs on our continent. As always, nothing that we would like to do would be possible with the participation of all of us, including you, the membership of the association, the directorship of each of the national societies, your representatives on the Board of Directors, and the Executive Committee of the association. With everyone's participation, we will contribute to an even better PanAmerica Association of Ophthalmology. A todos os membros da Associação Pan-Americana de Oftalmologia: ssumir a presidência da Associação Pan-Americana de Oftalmologia é provavelmente a maior honra a que pode aspirar um oftalmologista latino-americano. A APAO é uma organização supranacional que inclui, sem exceção, todos os países deste continente com três línguas oficiais e possui mais de 15.000 membros. É também, sem dúvida, dentre todas as organizações supranacionais existentes no mundo, a mais ativa e intensa. Como resultado, em seu gênero, é um modelo e aspiração das outras entidades supranacionais que se integram dentro do Concílio Internacional de Oftalmologia. Nossa associação se reúne de forma bienal e sem interrupções há mais de 50 anos. Acaba de concluir o XXV Congresso Pan-Americano realizado na cidade de Santiago, Chile. Mais de 2.500 oftalmologistas estiveram presentes. A organização foi perfeita graças ao esforço realizado pelo comitê organizador liderado brilhantemente pelo Dr Juan Verdaguer. As atividades do congresso se desenvolveram em um ambiente acadêmico, de interesse e cordialidade. O congresso em Santiago foi um prazer para todos aqueles que tiveram a oportunidade de participar. Os congressos pan-americanos são o ápice de nossa organização, na organização destes empreendemos muitos esforços e atenção, pois eles refletem fielmente o estado da Oftalmologia deste continente e são a A : 2 : VISIONPAN-AMERICA oportunidade que temos de nos apresentarmos, nos conhecermos e estreitarmos as amizades. A atividade acadêmica desenvolvida e de tal intensidade que em Santiago estiveram presentes mais de 1.200 oftalmologistas que ativamente apresentaram suas experiências e compartilharam conhecimentos. No próximo ano, em Fevereiro de 2006, em São Paulo, em conjunção com o Congresso Mundial de Oftalmologia, a APAO se juntará a esta organização, como parte integral do congresso e teremos a oportunidade de expor nossa Oftalmologia frente a todo o mundo em um ambiente único, pré-carnaval, na bonita cidade de São Paulo. Este será o XXVI Congresso de nossa associação. Par o ano de 2007, no mês de Maio em Cancun, México, voltaremos a nos reunir. Para isto o comitê organizador do XXVII Congresso Pan-Americano já se encontra trabalhando. Para o ano de 2009 foram propostas duas cidades de nosso continente; Cartagena na Colômbia e Punta Del Este no Uruguai. Em ambos os casos os comitês nacionais já começaram a integrar e a elaborar as suas propostas para que na assembléia dos diretores em Chicago, neste ano, se vote e se defina a sede do XXVIII Congresso Pan-Americano de Oftalmologia. Apesar dos congressos serem um componente muito importante de qualquer associação médica, na APAO eles não representam tudo. Nossa associação tem uma intensa atividade que engloba vários outros ramos. Anualmente se organizam cursos regionais, onde se revisam, com finalidades educativas, temas da atualidade. Com este intuito, nos reuniremos este ano em Tucumán, Argentina e em Chihuahua, México. Um comitê específico de nossa associação se encarrega destes cursos de curta duração. A associação está também ativa nas políticas regionais de prevenção da cegueira; na promoção de banco de olhos; nesta revista; na comunicação através da página eletrônica; na educação médica de nossos residentes; na organização de cursos básicos em oftalmologia; na gênese de políticas regionais, de relações profissionais e na formação de jovens oftalmologistas que serão os líderes de nossa profissão no futuro; no fornecimento de bolsas acadêmicas e de pesquisa; na Academia Americana de oftalmologia com cursos préacademia e de resumo do melhor apresentado nesta; na formação de paramédicos e em todas as atividades que podem ajudar a oftalmologia intercontinental a superar e desenvolverse. Em tudo isso, a Associação Pan-Americana de Oftalmologia está presente. Ao assumir a presidência da mesma, assumo também o compromisso de continuara fazendo tudo já descrito, que é muito bom. Começaremos por dar ênfase na educação e padrões das residências na América Latina. Para isto, neste ano, iniciaremos com um curso conjunto com o Internacional Council of Ophthalmology e a Associação de Professores Universitários de Oftalmologia (AUPO), dos estados Unidos, destinado a "Ensinar a ensinar" os responsáveis pelas residências em Oftalmologia do nosso continente. Como sempre, nada do que se quer fazer será possível sem a participação de todos nós, de vocês como membros titulares de nossa associação, das mesas diretivas de cada uma das sociedades nacionais, de seus representantes na assembléia do Board of Directors e do próprio comitê executivo da própria associação. Com a participação de todos conseguiremos uma melhor Associação Pan-Americana de Oftalmologia. Enrique Graue Presidente de la Asociación Panamericana de Oftalmología. President Pan-American Association of Ophthalmology. Presidente Associação Pan-Americana de Oftalmologia. Junio 2005 Leadership Development EDITORIAL by Zélia M Corrêa and Michael Brennan Leadership Development s we move into 2005, it is time to acknowledge the achievements and failures of 2004 in order to set the objectives for the future. We, from the PAAO's "Curso de Liderazgo" Committee and the recently created Leadership Committee, have a lot to be proud of at this time. The PAAO's "Curso de Liderazgo" that started as only a promise to develop future leaders is quickly becoming a reality, thanks to the hard work and support from the organizers, staff and PAAO Executive Committee. The first leadership class just graduated during the American Academy of Ophthalmology's Annual Meeting in New Orleans and the second class began their activities at the same time. The seeds planted by the "Curso" seem to be of good quality and fertile, since many graduates and current students are actively participating in their national societies, subspecialty societies and other professional related activities and community service. In addition, the results of the projects developed by the first class have already come to fruition in some Latin American and European countries such as Costa Rica, Puerto Rico, El Salvador, Venezuela, Dominican Republic, Chile, Brazil, Mexico, Portugal and Spain. These motivated colleagues have demonstrated the strength and energy of the future generation of leaders for Latin-American Ophthalmology. In light of this, there is nothing more appropriate than acknowledging those who are willing to prepare for the job: A 2003-2004 Class 2004-2005 Class José Manuel Benítez, MD, PhD Madrid, Spain Emilio A. Arce, MD San Juan, Puerto Rico Fernando L. Colombo, MD Caracas, Venezuela Fernando Barria, MD Concepcion, Chile José J. Flores-Rivera, MD Santa Tecla, El Salvador Javier Córdoba, MD San José, Costa Rica Natalio J. Izquierdo, MD San Juan, Puerto Rico Sergio Byron Deutschmann, MD Guatemala City, Guatemala Luis Izquierdo, Jr., MD Lima, Peru Marco A. De La Fuente, MD Mexico City, Mexico Miguel Angel López Pimentel, MD Sto Domingo, Dominican Republic H. Fernando Gómez, MD Bogotá, Colombia Paulo Henrique Morales, MD São Paulo, Brazil Lelia Marroquín, MD Lima, Peru Eduardo Silva, MD PhD Figueira da Foz, Portugal Francisco José Muñoz, MD Madrid, Spain José Luis Tovilla-Canales, MD Mexico City, Mexico Paola Pacheco, MD Montevideo, Uruguay Gonzalo Vargas, MD Santiago, Chile Karen Salcedo, MD Caracas, Venezuela Lihteh Wu, MD San José, Costa Rica Leon O Vaughan, MD Kingston, Jamaica As we set our plans for the future, it is important to invite every member of the PAAO to get involved. Find out what you can do for our profession and your community. But most of all encourage the young ophthalmologists of your country to join this program and become more active in your national society and the PAAO. Our past and current "Curso" participants are the best resource and information for their country's National Society. Remember that finding the right people for future "Curso de Liderazgo" classes is a challenge, However it is essential to keep this program successful and perpetuate the concept of speaking with ONE VOICE. Only then the echo of our ideas will be heard in every country of Latin America. On behalf of the Organizing Committee of the PAAO's Curso de Liderazgo, I would like to congratulate the first and second "Curso de Liderazgo" classes and all of those who participated, supported and/or contributed to this challenging project! Thank you for believing we can create a better professional environment in which we all care for our patients.. Rita A. Yee, MD Panama City, Panama VISIONPAN-AMERICA : 3 : Junio 2005 Interferon Alfa 2b in the Medical Management of Ocular Surface Squamous Neoplasia Aaleya F. Koreishi, MD and Carol L. Karp, MD Miami, Florida, U.S.A. Correspondence and Reprint Requests to: Carol L. Karp, MD, Bascom Palmer Eye Institute, University of Miami School of Medicine, 900 NW 17th Street, Miami, FL 33136 Neither of the authors has proprietary or financial interest in any product mentioned. ABSTRACT Interferons are glycoproteins that bind to cell-surface receptors and lead to anti-viral, anti-proliferative, and anti-angiogenic properties. Interferons have been used successfully in many different diseases throughout medicine, and recently success has been demonstrated for the treatment of ocular surface neoplasias. Traditional treatment for corneal and conjunctival intraepithelial neoplasia and squamous cell carcinoma includes surgical excision and adjunctive cryotherapy. The use of chemotherapeutic agents, including interferon alfa 2b (IFN a2b), mitomycin C (MMC) and 5-fluorouracil (5-FU), has limited the need for extensive surgical manipulation of the ocular surface and potentially decreases recurrence rates. This article will focus on the use of IFN in the treatment of corneal and conjunctival intraepithelial neoplasia and squamous cell carcinoma. INTERFERONS The Interferons (alpha, beta, and gamma) are a group of glycoproteins, produced naturally as part of an immunologic response, that bind to cell-surface receptors, and trigger an intracellular cascade resulting in antiproliferative, antiviral, immunomodulating and antiangiogenic properties1. The exact mechanism of action has not yet been elucidated2. Interferon Alfa 2b (IFN a2b) is a recombinant form of naturally occurring interferon-a. The United States Food and Drug Administration has approved IFN a2b for the treatment of chronic hepatitis B and C, AIDS-related Kaposi's sarcoma, malignant melanoma, hairy cell leukemia, chronic myelogenous leukemia, follicular lymphoma and condyloma accuminata. It has been used successfully in the treatment of squamous cell carcinoma and basal cell carcinoma of the skin3, as well as in cervical intraepithelial neoplasia. IFN a2b has been reported in the literature to be an effective treatment for ocular lesions including Herpes simplex keratitis4, Kaposi's sarcoma of the conjunctiva5, conjunctival MALT6, and Behcet's disease7. The anti-viral properties of IFN are evident by the successful use of IFN a2b in the treatment of herpes simplex keratitis (HSV), condyloma acuminate (HPV), and Kaposi's sarcoma (human herpes virus 8). Human papilloma virus (HPV) can infect cutaneous and mucosal epithelium and result in squamous cell tumors of the skin and intraepithelial neoplasia of the cervix8. HPV infection has also been demonstrated in association with conjunctival and corneal intraepithelial neoplasia (CIN) and squamous cell carcinoma (SCCA)9, 10, 11. The anti-viral properties of IFN a2b may play an important role in the response of HPV-associated CIN to this treatment. Although IFN therapy has shown promising results in the diseases discussed above, systemic use leads to many side-effects such as flu-like symptoms, hypotension, tachycardia, somnolence and anorexia.1 Local (subcutaneous or subconjunctival) injections may be associated with flu-like symptoms which can be controlled with acetaminophen12. Retinal cotton wool spots and vasculopathy was reported in one patient undergoing high-dose subcutaneous IFN a2b treatment for renal cell carcinoma13. Ocular topical drops are well tolerated, with only mild follicular conjunctivitis reported14. Corneal and Conjunctival Intraepithelial Neoplasia CIN is a pre-cancerous lesion on a continuum with SCCA. These tumors most commonly occur in older patients and tend to affect men more often than woman. Salient risk factors include ultraviolet light exposure15, 16 human papillomavirus infection (HPV),9,10,11 immunosuppression (HIV/AIDS)17, smoking, petroleum product exposure18, and genetic predisposition in conditions such as xeroderma pigmentosa19. Clinically, CIN presents as a gelatinous, papillomatous and/or Figure 1A Figure 1B leukoplakic growth on the ocular surface most commonly at the Figure 1: limbus in the interpalpebral zone (Figure 1) Corneal involvement 1A. Typical appearance of papillary, gelatinous CIN in the interpalpebral presents as a frosted-glass appearance with fimbriated edges zone. 1B. Leukoplakic CIN at the limbus. (Figure 2). SCCA tends to present as a larger, more elevated lesion with fixation to underlying sclera. Although some authors feel that the diagnosis of CIN/SCCA can be made reliably by clinical examination alone, pathologic confirmation is warranted, as other lesions may be confused with CIN/SCCA. The differential diagnosis includes pannus, pingueculae, nodular conjunctivitis/episcleritis, keratoacanthoma, and non-pigmented conjunctival nevi/melanoma. : 4 : VISIONPAN-AMERICA Junio 2005 phototherapeutic keratectomy34, and IFN a2b35, 36, 37, 38, 39, 40, 41, 42. The use of IFN a2b is appealing because it has fewer observed side-effects than other Figure 2A Figure 2B chemotherapeutic Figure 2: agents12, 43, IFN a2b 2A. Corneal involvement of CIN demonstrating fimbriated edges. 2B. used as a subconjuncLimbal CIN with both conjunctival and corneal components. The extent of corneal involvement can be appreciated with Rose Bengal tival injection and/or staining to delineate the fimbriated edges. as a topical drop has successfully treaTraditional treatment of CIN includes ted cases of primary and recurrent surgical excision with tumor-free margins. CIN/SCCA. It has also been used in Most surgeons now advocate the use of conjunction with other treatment modalities adjunctive cryotherapy to the limbus and or after treatment failure. The standard conjunctival margins in a double- or tripleformulations of topical drops (1 million freeze-slow-thaw technique20, 21. Erie et al22 units/ml) and subconjunctival injection (3 studied the recurrence of surgically treated million units/ml) are listed in Table 1. CIN in 98 patients. Eighty-two patients underwent surgical excision alone, 9 had Review of the literature adjunctive radiation, 6 had adjunctive thioTable 2 summarizes the available literature tepa, and one had an enucleation. The on the treatment of CIN/SCCA with IFN a2b. recurrence rate was 53% if surgical margins The first reported case in the English were positive and only 5% if the surgical literature35 demonstrated successful treatmargins were tumor-free. Similarly, Tabin et ment of a recurrent, pathologically-proven, al23 found that the main prognostic factor in epithelial dysplastic lesion of the conjunctiva determining recurrence is involvement of and cornea using only topical IFN a2b twice surgical margins. The rate of recurrence a day. The lesion regressed visibly after one was 39% overall, but 56% of incompletely week of treatment and the IFN a2b was excised lesions recurred, versus 33% of tapered over 2 months. No recurrence was completely excised lesions. In their study seen for 9 months. group, most patients underwent surgical The majority of initial reports described excision alone, four patients had radiation the use of subconjunctival/perilesional inadjunctively, and five patients underwent jection of IFN a2b with supplemental topical adjunctive cryotherapy to the limbus. A drops. Hu et al36 reported one case treated trend toward longer time to recurrence was with this combination. Impression cytology observed when adjunctive treatment was confirmed clinical suspicion, diagnosing rendered at the time of surgical excision. severe squamous dysplasia/CIN. As the 24 Peksayar et al reported low rates of recupatient refused surgical intervention, the rrence, in only 2 of 22 eyes (9%), when lesion was treated with 2 subconjunctival using adjunctive cryotherapy to the surgical injections, 1 week apart, and topical drops margins, limbus and episclera. One recufour times a day. Early regression was norrence was noted in the primary tumor ted at 3 weeks and the lesion resolved by 2 group and one out of 3 previously treated months. The drops were continued for 2 weeks. lesions recurred. They followed patients for No recurrence was noted for 10 months. 5 to 12 years, but both recurrences occuVann and Karp12 reported the largest series rred within 2 years. (6 eyes) of histologically proven CIN treated In eyes with recurrent disease, or with injection of IFN a2b followed by topical extensive tumor involvement, the surgical IFN a2b four times a day. The patients were approach may lead to significant ocular seen at 1 week, and if the lesion did not surface morbidity in terms of limbal stemdemonstrate regression, re-injection 3 times cell deficiency and scarring. Other treatper week was instituted. Overall, patients ment strategies have been tested in an required one to 11 injections, resolving attempt to limit surgical manipulation of the 25, 26 27 between 3 and 6 weeks. All patients , vitamin A , ocular surface: radiation 28, 29, 30, 31 32, 33 remained tumor-free for a follow up of 2-11 Mitomycin C , 5-fluorouracil , months. There appeared to be a dosedependent response, larger lesions requiring more injections. Kobayashi et al40 report a case of recurrent (after cryotherapy), histologically proven CIN treated with 2 subconjunctival injections, 1 week apart, and topical drops 4 times a day for 12 weeks. The lesion disappeared clinically by 2 weeks. Side effects included superficial punctuate keratopathy, which resolved after stopping the drops, and fever after the first injection, which was treated with Diclofenac. Subconjunctival IFN a2b injections may be used as a post-operative adjunct to subtotal excision of CIN in order to limit potential stem cell compromise and resulting ocular surface disease. Chen at al42 partially excised a large limbal lesion, involving 9 clock hours of limbus, positive for both HPV-16 and 18, and treated it with two injections 2 and 3 weeks postoperatively. The lesion regressed completely after 7 weeks. No evidence of recurrence was noted for 32 months. Interestingly, the patient's other eye also had a smaller CIN lesion which was totally excised initially, had no adjunctive IFN treatment, and recurred after 10 months. In order to minimize the side-effects from subconjunctival injections, several authors have reported the successful use of topical IFN a2b to treat CIN. Schechter37 described one case of extensive, recurrent CIN treated with topical IFN a2b for a total of 5 months, 4 times a day for 2 months followed by two times a day for three months. No recurrence occurred for the 19 month follow-up period. Karp et al38 reviewed their experience with topical IFN treatment of 5 eyes with histologically proven CIN. Duration of treatment ranged from 4 to 22 weeks (average, 12 weeks). One eye experienced a recurrence after 1 year and was retreated successfully over 6 weeks, with no recurrence for 8 months. After clinical improvement was noted, the drops were tapered in 3 patients, and discontinued without a taper in 2 patients. The follow up after treatment was between 7 and 28 months. The use of topical IFN a2b as the only therapy for presumed primary CIN was studied by Schechter et al39 in seven patients. The diagnosis was made clinically, as none of the patients underwent pathologic diagnosis. One patient was asked to increase the frequency to six times a day, VISIONPAN-AMERICA : 5 : Junio 2005 Table 1: Formulation of IFN a2b for Ophthalmic Use Interferon a2b 1 million units/ml From Bascom Palmer Pharmacy, Miami, FL. 1. Draw 0.83 ml from vial of INTRON A solution (18 million units/3ml) and Q.S. to 5 ml with Bacteriostatic Water for Injection, USP. 2. Transfer solution to 15 ml amber dropper bottle 3. Label, refrigerate, 30-day expiration date Interferon a2b 3 million units/ml From Bascom Palmer Pharmacy, Miami, FL. 1. Draw up 2.5 ml from vial of INTON A solution (18 million units/3ml) and Q.S. to 5 ml with Bacteriostatic Water for Injection, USP 2. Transfer solution to 15 ml amber dropper bottle. 3. Label, refrigerate, 30-day expiration date. Table 2: Summary of Literature Review on IFN a2b for CIN/SCCA Author Number of cases Tumor Description IFN a2b Treatment Time to Resolution Treatment Duration Tumor Free Follow-up Hu et al, 1998 1 Impression Cytology-severe dysplasia Injection x 2 and topical QID 2 months 2.5 months 10 months Early regression noted at 3 weeks. Vann and Karp, 1989 6 Histologyprimary CIN or recurrence of histologically proven CIN Injection (range, 3-6 weeks 1-11; average, (average, 4.5) 5) and topical QID 2-11 months (average, 7.2) Injection at start, then 3 X/week if no response at 1 week follow-up. Dosedependent response noted (larger lesions need more). Kobayashi et al, 2002 1 Histology-CIN, s/p cryo x 2 with recurrence Injection x 2 and topical QID 1 year Superficial punctuate keratopathy, resolved after stop drops, fever after injection, resolve with Diclofenac. Histologybilateral CIN, HPV 16, 18 Injection x 2 and Chen et al, 2004 1 (bilateral involvem ent) 2 weeks (clinical resolution) 12 weeks 7 weeks 32 months Comments Partial surgical excision, large lesion. IFN injections post-op. Other eye had complete excision without IFN treatment (recurred after 10 months). Maskin, 1994 1 Pathologyepithelial dysplasia Topical BID 2 months 9 months Schechter, 1999 1 Extensive recurrent CIN Topical QID 2 months, BID 3 months 5 months 19 months Karp et al, 2001 5 Histology-CIN Topical QID (tapered in 3pt, stopped in 2pts) 4-22 weeks (average 11.6) 7-28 months (average 17.6) 1 eye recurred after 1 year, re-treated 6 weeks, no recurrence 8 months. Schechter et al, 2002 7 Clinical CIN Topical QID (1 18-188 days pt increased to (average, 77) 6x a day after 8 wks, 1 pt started on 6 x a day) 57-188 days (average, 106) 9-18 months (average, 14) 4/7 patients with follicular conjunctivitis. Boehm and Huang, 2004 7 Clinical Topical QID diagnosis of recurrent CIN (# of recurrences: 1, 2, 2, 3, 6) 6-24 weeks (average, 14.1) 8-17 months (average, 11.7) Initial treatment was surgical excision, cryotherapy, radiation and/or topical MMC. Regression noted at 2 weeks.First case reported. Junio 2005 as no regression was noted after 8 weeks. Another patient was started at 6 times per day. Similar to Karp, resolution occurred after an average of 77 days and total treatment averaged 106 days. Four out of the seven patients experienced follicular conjunctivitis, which generally lead to earlier discontinuation of the drops. No clinical recurrences were noted over an average of 14 months. Recently, recurrent CIN lesions and their response to topical IFN a2b were reported by Boehm and Huang.41 All patients had undergone surgery, cryotherapy, radiation and/or topical MMC treatment, and pathologic diagnosis of their primary lesion. Three patients had 1 recurrence, 2 patients had 2 recurrences, one patient had 3 recurrences, and one patient had 6 recurrences. Of the seven patients studied, 6 had a clinical resolution in an average of 14.5 weeks. The treatment was continued for 14.1 weeks. Although one patient developed a recurrent lesion at a different site and was restarted on treatment, the tumor-free follow-up period for the others averaged 11.7 months. Summary/ Clinical significance Indications of use The gold standard includes surgical excision and adjuvant cryotherapy as the primary treatment option. The role of adjuvant chemotherapy or chemotherapy as a primary treatment is especially helpful for lesions demonstrating recurrence, large, annular limbal lesions which might lead to limbal stem cell def, non-resectable lesions, and, and lesions in patients who are not surgical candidates (although confirmatory pathologic diagnosis is still recommended). IFN a2b is one of the available choices for adjuvant treatment. Treatment protocol Use of subconjunctival IFN a2b (3 million U/ml, 0.5cc, Scherring Plough, NJ) with topical drops (1 million units/ml): Large lesions, multiple recurrences after extensive ocular surface surgery, and patients who want a potentially quicker recovery may be treated with subconjunctival injections. The injections can be given 1 week apart and up to 3 times per week. The patient is monito-red for response. Once the tumor has resolved, the injections are stopped and topical Figure 3A Figure 3B Figure 3: 3A. CIN before treatment. 3B. Resolution of CIN after treatment with IFNa2b injections and topical drops. Figure 5A Figure 5B Figure 5: 5A. Corneal CIN pre-treatment. (Pending permission from Ophthalmology). 5B. Resolution after 7 weeks of topical IFN a2b treatment. (Pending permission from Ophthalmology) drops are continued for one month. Figures 3 and 4 demonstrate clinical appearance of CIN lesions treated with this protocol. Use of topical IFN a2b (1 million units/ml): Smaller lesions may be treated with topical drops alone. The usual frequency is four times a day, although clinicians have increased to 6 times a day dosing if sufficient regression is not noted, or if the lesion is very large. The drops are usually continued through complete tumor resolution and may be tapered afterwards. Discontinuation after a set period of time (1 month) after tumor resolution has also been successful. This decision may be made depending on the initial size of the lesion, time to response, and side effects. Figure 5 shows the clinical resolution of corneal CIN after topical IFN a2b treatment. Side-effects Although side-effects have been reported, IFN a2b has a milder side-effect profile than the other chemotherapeutic options inclu-ding MMC and 5-FU. The only systemic side-effect reported during ocular use of subcon-junctival injections is fever and chills, which is transient and treated with acetaminophen. Topical IFN a2b may elicit a follicular con-junctivitis, or superficial punctuate keratitis. Both of these side-effects resolve after cessation of the medication. CONCLUSION IFN a2b provides a valuable tool against ocular surface neoplasia, specifically CIN/SCCA. Although surgical excision with adjunctive cryotherapy continues to be the gold standard for most CIN/SCCA, indi-vidual patient circumstances may warrant a less invasive approach. Topical treatment with IFN a2b is ideal for patients who have a compromised ocular surface, who are not good surgical candidates or who do not want invasive procedures, if the lesion size is relatively small or mostly corneal. As topical treatment seems to take longer to reach tumor resolution, subconjunctival injections may be more effective for larger lesions. The use of IFN a2b in ophthalmology is only just becoming apparent and future investigation will best determine the ideal dosing regiment. Further long term studies are needed to better assess recurrence rates and other adverse effects, and to prospectively compare results to surgical excision. Figure 4A Figure 4B Figure 4: 4A. Leukoplakic CIN before treatment. 4B. Appearance after 4 injections of IFN a2b with concomitant topical drops. Junio 2005 1. Baron S, Tyring SK, Fleischmann WR, Coppenhaver DH, Niesel DW, Klimpel GR, Stanton GJ, Hughes TK. The interferons. mechanism of action and clinical applications. JAMA, 1991; 266(10): 1375-1383. 2. Parmar S, Plantanias LC. Interferons: mechanism of action and clinical applications. Curr Opin Oncol, 2003; 15(6): 431-439. 3. Kim KH,Yavel RM, Gross VL, Brody N. Intralesional interferon a2b in the treatment of basal cell carcinoma and squamous cell carcinoma: revisited. Dermatol Surg, 2004; 30(1): 116-120. 4. Minkovitz JB, Pepose JS. Topical interferon alpha 2a treatment of herpes simplex keratitis resistant to multiple antiviral medications in an immunosuppressed patient. Cornea, 1995: 14(3): 326-330. 5. Hummer J, Gass JD, Huang AJW. Conjunctival Kaposi's sarcoma treated with interferon alfa 2a. Am J Ophthalmol, 1993: 116(4): 502-503. 6. Blasi MA, Gherlinzoni F, Calvisi G, Sasso P, Tani M, Cellini M, Balestrazzi E. Local therapy with interferon a for conjunctival mucosaassociated lymphoid tissue lymphoma. A preliminary report. Ophthalmology, 2001; 108(3): 559-562. 7. Kotter I, Eckstein AK, Stubiger N, Zierhut M. Treatment of ocular symptoms of Behcet's disease with interferon alpha 2a: a pilot study. Br J Ophthalmol, 1998; 82(5): 488-494. 8. Bornstein J, Rahat MA, Abramovici H. Etiology of cervical cancer: current concepts. Obstet Gynecol Surv, 1995; 50(2): 146-154. 9. Scott IU, Karp CL, Nuovo GJ. Human papillomavirus 16 and 18 expression in conjunctival intraepithelial neoplasia. Ophthalmology, 2002; 109(3): 542-547. 10. Karcioglu ZA, Issa TM. Human papilloma virus in neoplastic and nonneoplastic conditions of the external eye. Br J Ophthalmol, 1997; 81(7): 595-598. 11. McDonnell JM, McDonnell PJ, Sun YY. Human papillomavirus DNA in tissues and ocular surface swabs of patients with conjunctival epithelial neoplasia. Invest Ophthalmol Vis Sci, 1992; 33(1): 184-189. 12. Vann RR, Karp CL. Perilesional and topical interferon alfa 2b for conjunctival and corneal neoplasia. Ophthalmology, 1999; 196(1): 91-97. 13.Hoerauf H, Schmidt-Erfurth U, Asiyo-Vogel M, Laqua H. Combined choroidal and retinal ischemia during interferon therapy: indocyanine green angiographic and microperimetric findings. Arch Ophthalmol, 2000; 118(4): 580-582. 14.BSmith M, Trousdale MD, Rao NA, Robin JB. Lack of toxicity of a topical recombinant interferon a. Cornea, 1989; 8(1): 58-61. 15.Lee GA, Williams G, Hirst LW, Green AC. Risk factors in the development of ocular surface epithelial dysplasia. Ophthalmology, 1994;101(2): 360-364. 16.Tulvatana W, Bhattarakosol P, Sansopha L, Sipiyarak W, Kowitdamrong E, Paisuntornsug T, Karnsawai S. Risk factors for conjunctival squamous cell neoplasia: a matched case-control study. Br J Ophthalmol, 2003; 87(4): 396-398. 17.Newton R, Ziegler J, Ateenyi-Agaba C, Bousarghin L, Casabonne D, Beral V, Mbidde E, Carpenter L, Reeves G, Parkin DM, Wabinga H, Mbulaiteye S, Jaffe H, Bourboulia D, Boshoff C, Touze A, Coursaget P; Uganda Kaposi's Sarcoma Study Group. The epidemiology of conjunctival squamous cell carcinoma in Uganda. Br J Cancer. 2002; 87(3): 301-308. 18.Napora C, Cohen EJ, Genvert GI, Presson AC, Arentsen JJ, Eagle RC, Laibson PR. Factors associated with conjunctival intraepithelial neoplasia: a case control study. Ophthalmic Surg, 1990; 21(1): 27-30. 19.Goyal JL, Rao VA, Srinivasan R, Agrawal K. Oculocutaneous manifestations in xeroderma pigmentosa. Br J Ophthalmol, 1994; 78(4): 295-297. 20.Peksayar G, Altan-Yaycioglu R, Onal S. Excision and cryosurgery in the treatment of conjunctival malignant epithelial tumors. Eye, 2003;17(2): 228-32. 21.Singh AD. Excision and cryosurgery of conjunctival malignant epithelial tumors. Eye, 2003; 17(2): 125-126. : 8 : VISIONPAN-AMERICA 22.Erie JC, Campbell RJ, Liesegang TJ. Conjunctival and corneal intraepithelial and invasive neoplasia. Ophthalmology, 1986; 93(2): 176-183. 23.Tabin G, Levin S, Snibson G, Loughnan M,Taylor H. Late recurrences and the necessity for long-term follow-up in corneal and conjunctival intraepithelial neoplasia. Ophthalmology, 1997; 104(3): 485-492. 24.Peksayar G, Soyturk MK, Demiryont M. Long-term results of cryotherapy on malignant epithelial tumors of the conjunctiva. Am J Ophthalmol, 1989; 107(4): 337-40. 25.Cerezo L, Otero J, Aragon G, Polo E, de la Torre A,Valcarcel F, Magallon R. Conjunctival intraepithelial and invasive squamous cell carcinomas treated with strontium-90. Radiother Oncol, 1990; 17(3): 191-197. 26.Kearsley JH, Fitchew RS, Taylor RG. Adjunctive radiotherapy with strontium-90 in the treatment of conjunctival squamous cell carcinoma. Int J Radiat Oncol Biol Phys, 1988; 14(3): 435-443. 27.Herbort CP, Zografos L, Zwingli M, Schoeneich M. Topical retinoic acid in dysplastic and metaplastic keratinization of corneoconjunctival epithelium. Graefes Arch Clin Exp Ophthalmol, 1988; 226(1): 22-26. 28.Frucht-Pery J, Rozenman Y. Mitomycin C therapy for corneal intraepithelial neoplasia. Am J Ophthalmol, 1994; 117(2): 164-168. 29.Wilson MW, Hungerford JL, George SM, Madreperla SA. Topical mitomycin C for the treatment of conjunctival and corneal epithelial dysplasia and neoplasia. Am J Ophthalmol, 1997; 124(3): 303-311. 30.Frucht-Pery J, Sugar J, Baum J, Sutphin JE, Pe'er J, Savir H, Holland EJ, Meisler DM, Foster JA, Folberg R, Rozenman Y. Mitomycin C treatment for conjunctival-corneal intraepithelial neoplasia: a multicenter experience. Ophthalmology, 1997; 104(12): 2085-2093. 31.Shields CL, Naseripour M, Shields JA.Topical mitomycin C for extensive, recurrent conjunctival-corneal squamous cell carcinoma. Am J Ophthalmol, 2002; 133(5): 601-606. 32.Yeatts RP, Ford JG, Stanton CA, Reed JW. Topical 5-fluorouracil in treating epithelial neoplasia of the conjunctiva and cornea. Ophthalmology, 1999; 102(9): 1338-1344. 33.Midena E, Angeli CD, Valenti M, de Belvis V, Boccato P. Treatment of conjunctival squamous cell carcinoma with topical 5-fluorouracil. Br J Ophthalmol, 2000; 84(3): 268-272. 34.Dausch D, Landesz M, Schroder E. Phototherapeutic keratectomy in recurrent corneal intraepithelial dysplasia. Arch Ophthalmol, 1994; 112(1): 22-23. 35.Maskin SL. Regression of limbal epithelial dysplasia with topical interferon. Arch Ophthalmol, 1994; 112(9): 1145-1146. 36.Hu FR,Wu MJ, Kuo SH. Interferon treatment for corneolimbal squamous dysplasia. Am J Ophthalmol, 1998; 125(1): 118-119. 37.Schechter BA. Conjunctival intraepithelial neoplasia. Ophthalmology, 1999; 106(9): 1642-1643. 38.Karp CL, Moore JK, Rosa RH Jr. Treatment of conjunctival and corneal intraepithelial neoplasia with topical interferon alpha-2b. Ophthalmology, 2001; 108(6): 1093-1098. 39.Schechter BA, Schrier A, Nagler RS, Smith EF, Velasquez GE. Regression of presumed primary conjunctival and corneal intraepithelial neoplasia with topical interferon alpha-2b. Cornea, 2002; 21(1): 6-11. 40.Kobayashi A,Yoshita T, Uchiyama K, Shirao Y, Kitagawa K, Fujisawa A,Tseng SC. Successful management of conjunctival intraepithelial neoplasia by interferon alpha-2b. Jpn J Ophthalmol, 2002; 46(2): 215-217. 41.Boehm MD, Huang AJ. Treatment of recurrent corneal and conjunctival intraepithelial neoplasia with topical interferon alfa 2b. Ophthalmology, 2004; 111(9): 1755-1761. 42.Chen HC, Chang SW, Huang SF. Adjunctive treatment with interferon alpha-2b may decrease the risk of papilloma-associated conjunctival intraepithelial neoplasm recurrence. Cornea, 2004; 23(7): 726-729. 43.Smith M,Trousdale MD, Rao NA, Robin JB. Lack of toxicity of a topical recombinant interferon alpha. Cornea, 1989; 8(1): 58-61. Junio 2005 Ceratite pelo vírus Herpes simples Denise de Freitas, MD UNIFESP/EPM Rua Botucatu, 822 CEP 04023-062 São Paulo, SP, Brasil [email protected] A autora não tem interesse financeiro no assunto. INTRODUÇÃO O vírus herpes simples (HSV) causa uma infecção primária que é, na grande maioria das vezes, assintomática e auto-limitada. O HSV é um importante agente etiológico das ceratites, podendo se manifestar na forma infecciosa e imunológica, as quais requerem tratamentos específicos e diferentes entre si. O pronto reconhecimento e tratamento de cada manifestação diminuem a morbidade da doença. Manifestações clínicas e tratamento das diferentes formas de ceratite herpética As manifestações clínicas da doença herpética ocular no segmento anterior do olho podem ser didaticamente divididas em: 1. Doença ocular primária: manifesta-se mais freqüentemente como vesícu-las ao redor do olho (Figura 1), com ou sem concomitante envolvimento da conjuntiva e da córnea. Estas vesículas ulceram e evoluem para crostas em um prazo médio de 7 dias. O tratamento da infecção primária é controverso por tratar-se de uma infecção auto-limitada e benigna na grande maioria dos casos. Nos recomendamos que o tratamento das lesões de pele próximas ao olho, principalmente aquelas com acometimento das pálpebras (blefarite), seja feito com antiviral tópico local na pele e no olho, com dosagem terapêutica. Na tabela 1 podemos obFigura 1: servar os antivirais de uso tópico utilizados no tratamento da infecção ocular pelo herpes simples e respectivas posologias terapêuticas e profiláticas.Lesões extensas de pele ou múltiplos focos de acometimento podem ser tratados com antiviral sistêmico (Tabela 2). Orientamos, também, a limpeza das lesões de pele com sabonete neutro. Tabela 1. Antivirais de uso tópico utilizados no tratamento da infecção ocular pelo herpes simples. CONCENTRAÇÃO, APRESENTAÇÃO DOSAGEM TERAPÊUTICA* DOSAGEM PROFILÁTICA Trifluoridina 1,0%, gotas 9x/dia 4-5x/dia Trifluoridina 1,0%, pomada 5x/dia 2-3x/dia Aciclovir 3,0%, pomada 5x/dia 2-3x/dia Idoxuridina 0,1%, gotas 9x/dia 4-5x/dia Idoxuridina 0,5%, pomada 5x/dia 2-3x/dia Vidarabina 3,0%, pomada 5x/dia 2-3x/dia DROGA * período de tratamento de 7 a 14 dias, conforme a necessidade, podendose diminuir a freqüência caso seja observado sinal de toxicidade Tabela 2. Antivirais de uso sistêmico para o tratamento da infecção pelo herpes simples DROGA APRESENTAÇÃO (COMPRIMIDOS) DOSAGEM TERAPÊUTICA* DOSAGEM (ADULTO) Aciclovir 1,0%, gotas 9x/dia 4-5x/dia Valaciclovir 1,0%, pomada 5x/dia 2-3x/dia Fanciclovir 3,0%, pomada 5x/dia 2-3x/dia *posologia extrapolada do tratamento do herpes genital. VISIONPAN-AMERICA : 9 : Junio 2005 2. Doença ocular recorrente: Podem manifestar-se nas formas de blefarite, conjuntivite, ceratite e uveíte. O acometimento corneano pode ser classificado em: 2.1. Ceratite Epitelial: Causada pela ação direta do vírus vivo replicando no epitélio da córnea. Pode iniciar-se com uma ceratite ponteada que evolui par a formação de linhas e figuras clássicas de dendritos (Figura 2) e úlceras em formato de mapas geográficos (Figura 3). Estas lesões são melhor observadas com o uso de rosa bengala. O dendrito da infecção pelo herpes simples é geralmente central, único (mas podendo ser múltiplo), apresenta ramificações com, classicamente, bulbo terminal. A lesão epitelial geográfica é o dendrito que perdeu seu padrão linear estendendo-se na forma de úlcera. Tem as bordas geralmente edemaciadas e que coram com rosa bengala. O tratamento da ceratite epitelial inclui o debridamento (com um cotonete seco retiram-se todas as células que coram com a rosa bengala) e a introdução do antiviral tópico (Tabela 1). 2.2. Ceratopatia Neurotrófica: São ulcerações do epitélio corneano, de fundo transparente, de formato ovóide ou arredondado, localizadas geralmente no centro da córnea e que apresentam as bordas elevadas devido ao empilhamento do epitélio (Figura 3) que fica impossibilitado de se deslizar para promover a cicatrização da úlcera. Quando crônicas, podem apresentar um estroma mais opaco, de coloração acizentada, assim como neovascularização superficial em formato de coroa ao redor da úlcera ("pannus" que tenta cicatrizar a lesão). Nestas úlceras mais crônicas é importante afastar a suspeita de infecção secundária através da pesquisa laboratorial. A ceratopatia neurotrófica herpética é secundária a má inervação corneana entre outros fatores como comprometimento do filme lacrimal, toxicidade medicamentosa, alteração e inflamação da membrana basal etc. A escolha do tratamento mais apropriado vai depender do tamanho, gravidade, tempo de aparecimento da ulceração e das outras tentativas de tratamento já efetuadas. Pode variar desde tratamentos clínicos não intervencionistas como lubrificação intensa, curativo oclusivo e lente de contato : 10 : VISIONPAN-AMERICA terapêutica, até procedimentos cirúrgicos como tarsorrafia (ou provocação de ptose pela aplicação de toxina botulínica), obstrução de pontos lacrimais e recobrimento conjuntival. O uso de membrana amniótica como tecido para recobrimento tem sido avaliado em nosso Serviço em caracter experimental. 2.3. Ceratite Estromal: São controversas em relação à fisiopatologia (manifestação de cunho imunológico e ou inflamatório não específico e ou infeccioso viral ativo). As ceratites estromais são classificadas em: 2.3.1. ceratite estromal necrosante: Provável invasão do estroma por infecção viral ativa com desencadeamento de inflamação. Clinicamente apresenta-se com ulceração, necrose do tecido corneano e densa infiltração estromal (Figura 4). Estes casos tendem a evoluir com afinamento, formação de descemetocele e perfuração. 2.3.2. ceratite estromal imune: Provavelmente um processo imunológico primário. Clinicamente o estroma pode apresentar-se com inflamação, de leve a severa, na forma de infiltração focal, multifocal ou difusa (Figura 5). O epitélio é geralmente íntegro com exceção nos casos de associação de ceratite epitelial (infecção viral ativa) ou ceratopatia neurotrófica. Uma outra manifestação da ceratite estromal imune é o anel imunológico que pode apresentar-se na forma de anel único ou múltiplo, completo ou incompleto, de infiltrado e edema de intensidade variável. Outro achado freqüente desta ceratite é a neovascularização que pode ocorrer em qualquer nível da córnea e nos casos de infiltração severa desenvolve-se com maior rapidez. A neovascularização também pode se desenvolver as custas de inflamação crônica de baixa intensidade. As ceratites estromais herpéticas são tratadas dependendo da severidade e localização da inflamação na córnea e da perda de tecido. Se a ceratite não envolve o eixo visual, não há neovascularização cor-neana e o olho encontra-se calmo opta-se pela observação prescrevendo-se lubrificantes e ou cicloplégicos para promover um melhor conforto para o paciente. Se a reação inflamatória é severa, localizada próxima ou no ao eixo visual e a Figura 2 Figura 3 Figura 4 Figura 5 Junio 2005 neovascularização é presente ou mostra sinais de desenvolvimento, opta-se pelo uso de corticóide. O tipo e freqüência do corticóide vão depender da severidade da inflamação. Deve-se fazer a profilaxia antiviral quando se usa corticóide no tratamento da ceratite herpética para evitar a recorrência da infecção epitelial viral ativa. Esta profilaxia fica na dependência do tipo e freqüência do corticóide utilizado. A redução do corticóide deve ser feita lentamente e na dependência da resposta clínica, recorrência da inflamação, tolerância e efeitos colaterais em relação ao colírio. Não se deve diminuir em mais do que 50% a freqüência de uso do corticosteróide tópico para evitar-se o efeito rebote da inflamação (termo em inglês conhecido como "flare dose"). É importante lembrar que os corticosteróides são totalmente contra-indicados na vigência de infecção epitelial herpética ativa. Eles não aumentam a incidência de recorrência da ceratite epitelial viral mas, se esta ocorrer, será agravada pelo seu uso uma vez que os corticosteróide promovem a replicação viral. Existem autores que preferem iniciar o tratamento da ceratite estromal herpética com uma dosagem baixa de corticosteróide tópico que é aumentada conforme a necessidade. Outros preferem iniciar com uma dosagem mais alta reduzindo-a conforme a melhora clínica. A Tabela 3 exemplifica o nosso sistema de uso do corticosteróide tópico, que deve ser feito sempre com profilaxia antiviral, quer seja tópica ou sistêmica, no tratamento das ceratites estromais herpéticas. 2.4. Endotelite: Reação inflamatória primária no endotélio corneano, sendo que um componente infeccioso de replicação viral ativa pode estar implicado na fisiopatogenia da inflamação. Pode apresentar-se na forma difusa, linear ou de disco (Figura 6), com precipitados ceráticos atrás da lesão ou em forma de linha, com edema estromal e algumas vezes epitelial e, em algumas casos, irite. Estes olhos são geralmente calmos, sem qualquer sinal inflamatório (hiperemia, lacrimejamento etc) e a córnea freqüentemente não desenvolve neovascularização. O tratamento, como na ceratite estromal, inclui o uso de corticóide (Tabela3) e antiviral sistêmico (Tabela 2). Em especial, casos onde há infecção epitelial Tabela 3. Uso do corticóide tópico no tratamento das ceratites estromais herpéticas. Semana Dexametasona 0,1% ou Prednisona 1,0% 1 8x/dia 2 6x/dia 3 4x/dia 4 5 2x/dia 1x/dia Semana Dexametasona 0,005% ou Prednisona 0,1% 6 7 4x/dia 3x/dia 8 2x/dia 9 1x/dia 10 3x/semana viral e inflamação estromal associadas, devese tratar primeiro a infecção epitelial e somente após o controle iniciar o uso do corticosteróide tópico. Quando há a associação de ceratopatia neurotrófica e inflamação estromal, deve-se primeiro fechar o defeito epitelial e depois desinflamar o estroma com o uso cauteloso do corticosteróide. A indicação do uso de antiviral oral ainda é controversa em algumas manifestações da doença ocular herpética. Existe uma tendência de concordância em se prescrever o antiviral oral nos casos de [1] infecção primária extensa e severa, [2] em casos selecionados de ceratouveíte, endotelite, iridociclite e trabeculite, [3] pacientes imunocomprometidos, nas profilaxias [4] de pacientes com doença ocular herpética com alta freqüência de recorrência e [6] nos pacientes submetidos a transplante de córnea. Figura 6 REFERENCES 1. Dawson, C., et al., Design and organization of the herpetic eye disease study (HEDS). Curr Eye Res, 1991. 10(105): p. 10. 2. Dawson, C., et al., Herpetic Eye Disease Study.You can help. Arch Ophthalmol, 1996. 114(1): p. 89-90. 3. Wilhelmus, K., et al., Herpetic Eye Disease Study. A controlled trial of topical corticosteroids for herpes simplex stromal keratitis. Ophthalmology, 1994. 101(12): p. 1883-95. 4. Barron, B., et al., Herpetic Eye Disease Study. A controlled trial of oral acyclovir for herpes simplex stromal keratitis. Ophthalmology, 1994. 101(12): p. 1871-82. 5. Anonymous, A controlled trial of oral acyclovir for iridocyclitis caused by herpes simplex virus. The Herpetic Eye Disease Study Group. Arch Ophthalmol, 1996. 114(9): p. 1065-72. 6. Wilhelmus, K., et al., Risk factors for herpes simplex virus epithelial keratitis recurring during treatment of stromal keratitis or iridocyclitis. Herpetic Eye Disease Study Group. Br J Ophthalmol, 1996. 80(11): p. 969-72. 7. Anonymous, A controlled trial of oral acyclovir for the prevention of stromal keratitis or iritis in patients with herpes simplex virus epithelial keratitis. The Epithelial Keratitis Trial. The Herpetic Eye Disease Study Group. Arch Ophthalmol, 1997. 115(9): p. 1196. 8. Anonymous, Acyclovir for the prevetion of recurrent herpes simplex virus eye disease. Herpetic Eye Disease Study Group. N Engl J Med, 1998. 339(5): p. 300-6. 9. Moyes, A., Antiviral therapy after penetrating keratoplasty for herpes simplex keratitis. Arch Ophthalmol, 1994. 112: p. 601-607. 10. Beyer, C., et al., Oral acyclovir reduces the incidence of recurrent herpes simplex keratitis in rabbits after penetrating keratoplasty. Arch Ophthalmol, 1989. 107(8): p. 1200-5. 11. Foster, C. and N. Barney, Systemic acyclovir and penetrating keratoplasty for herpes simplex keratitis. Doc Ophthalmol, 1992. 80(4): p. 363-9. 12. vanRooij, J., et al., A retrospective study on the effectiveness of oral acyclovir to prevent herpes simplex recurrence in corneal grafts. Eur J Ophthalmol, 1995. 5(4): p. 214-8. 13. Kaufman, HE., Varnell, ED., Thompson, HW. Trifluridine, cidofovir, and penciclovir in the treatment of experimental herpetic keratitis. Arch Ophthalmol, 1998. 116:6 p. 777-80. VISIONPAN-AMERICA : 11 : Junio 2005 Aspectos Genéticos y Oftalmológicos del Síndrome de Axenfeld Rieger Rodolfo A. Pérez Grossmann, MD Instituto de Glaucoma y Catarata Lima-Perú E n 1920 Axenfeld describió por primera vez un paciente con una línea blanca en la parte posterior de la cornea periférica que lo denomino embriotoxon posterior de la córnea (1). En 1935 Rieger reportó casos con alteraciones similares pero asociado a alteraciones del iris como corectopia, atrofia de iris con formación de agujeros; definiéndolo como disgenesias mesodermales de la cornea y del iris (2). Tradicionalmente se han designado tres condiciones: - Anomalía de Axenfeld, limitada a alteraciones periféricas del segmento anterior. - Anomalía de Rieger, con alteraciones periféricas del segmento anterior y alteraciones del iris. - Síndrome de Rieger, con alteraciones oculares y extraoculares. El Síndrome de Axenfeld Rieger representa un amplio espectro de alteraciones del desarrollo del segmento anterior del ojo y también alteraciones extraoculares, debido a la alteración en la formación de estructuras originadas en las células de la cresta neural. El compromiso ocular es bilateral y la alteración es asimétrica, quiere decir que puede existir compromiso en diferente grado en el mismo paciente y frecuentemente esta asociado a glaucoma. Los defectos extraoculares más comúnmente comprometen los dientes y los huesos faciales. GENÉTICA Esta alteración ocurre en aproximadamente 1 de cada 10,000 niños nacidos vivos (3). Es un defecto autosómico dominante con un espectro amplio de fenotipos que depende del grado de expresión de uno o más genes relacionados con la formación del segmento anterior. En algunos casos asociados a malformaciones sistémicas, particularmente a nivel de los dientes y huesos de la cara. Se han descrito tres locus y dos genes asociados a este síndrome: El primer gen ha sido descrito en el año 1997, el PITX 2 en el cromosoma 4q25 responsable del síndrome de Rieger tipo 1; posteriormente fue descrito el segundo locus para el síndrome de Rieger (RIEG2) en el cromosoma 13q14 mediante análisis de ligación genética y finalmente en el año 1998 el gen FOXC1 o FKHL7 fue implicado en un forma dominante de glaucoma congénito que revelo posteriormente ser responsable del síndrome de Axenfeld Rieger estando ubicado en el cromosoma 6p25. Asimismo en América Latina se ha descrito una mayor ligación genética al gen PITX 2 en la población brasilera (4). Mutaciones en estos genes pueden causar una variedad de fenotipos que comparten cuadros característicos con el síndrome de Axenfeld-Rieger; como son: la anomalía de Axenfeld, anomalía de Rieger, Síndrome de Rieger, anomalía : 12 : VISIONPAN-AMERICA o síndrome de iridodisgenesia, hipoplasia de iris y el glaucoma familiar por iridodisplasia (5). Asimismo las mutaciones PITX2 se asocian a una alta incidencia de glaucoma (6), que podría estar producido por mutaciones puntuales o microdelecciones del gen PITX2, para lo cual el PCR cuantitativo seria de mucha ayuda en estos pacientes para su detección(7).Todos comparten una sobre posición genotípica y fenotípica (8), con un 50% de riesgo de desarrollar glaucoma. Genes relacionados al síndrome de Rieger: El PITX2 ó RIEG I en el cromosoma 4p25 El FKHL7 o FOXC1 en el cromosoma 6p25 ALTERACIONES OCULARES Las estructuras mas comúnmente comprometidas son: La córnea periférica, el seno camerular y el iris. CORNEA En la córnea periférica se observa una línea de Schwalbe prominente y desplazada anteriormente. A la biomicroscopía se observa como un anillo de color blanquecino en la parte posterior de la cornea periférica, cerca al limbo. En algunos casos se limita solo a la región temporal y en otros se puede observar en los 360 grados de la cornea periférica (fotos 1 y 2). Junio 2005 En algunos casos puede existir esta línea de Schwalbe prominente, como un defecto aislado referido solo como embrio-toxon posterior (9), el cual se puede observar en alrededor de el 8 al 15% de la población general. Usualmente la córnea es de apariencia normal, pudiendo estar ocasionalmente asociado a megalocórnea, a microcórnea (10) o a opacidades de la córnea central. El endotelio corneal es normal a la microscopía especular, pudiendo estar alterada en su forma y tamaño en los glaucomas de larga data o con cirugía previa (11). Impreso por Printer Colombiana S.A. SENO CAMERULAR En la gonioscopía se observa típicamente una prominencia de la línea de Schwalbe cuya extensión y desplazamiento anterior es variable, en algunos casos se nota como suspendida de la córnea (12) (Foto 2). Prolongaciones el iris periférico a la línea de Schwalbe prominente que forman una especie de puentes y en algunas áreas con inserción en la malla trabecular. En algunos pacientes se observa una o dos prolongaciones del iris, mientras que en otras llega a tapizar casi por completo la malla trabecular con la presencia de algunas áreas libres. Debajo de estas pro-longaciones anómalas del iris se encuentra un ángulo abierto con una malla trabecular que se aprecia en algunas áreas libres. El espolón escleral esta oculto por el iris periférico el cual se inserta en la porción posterior de la malla trabecular (13). Foto 1: Se observa el embriotoxon posterior (Flecha negra), como una línea blanquecina en la cornea periférica en los 360 grados. Obsérvese también la pupila ubicada excéntricamente. Foto 2: Vista del embriotoxon posterior o prominencia de la línea de Schwalbe al corte de la lámpara de hendidura (Flecha blanca). Foto 3 y 4: Se observa la línea de Schwalbe prominente, con prolongaciones del iris periférico a la línea de Schwalbe o embriotoxon posterior (Flecha); detrás del cual se observa la malla trabecular. VISIONPAN-AMERICA : 13 : Preserva la visión alcanzando las menores presiones-objetivo en más pacientes Investigadores de diversos estudios, (AGIS, Shirakashi, Shields) han comprobado que alcanzar y mantener la PIO entre 14 y 15 mmHg reduce la progresión de pérdida del campo visual1,2,3. Lumigan® alcanza la PIO-objetivo de 14/15 mmHg en un mayor número de pacientes: ® vs. timolol 4 ® vs. dorzolamida/ timolol 5 ® vs. latanoprost 6 Porcentaje de Pacientes que alcanzaron la PIO-Objetivo ≤14 21% 9% 17% 2% 19% 9% Porcentaje de Pacientes que alcanzaron la PIO-Objetivo ≤15 31% 16% 24% 9% 29% 14% Lumigan ® (bimatoprost) Forma farmacéutica y pr esentación. Composición. Cada ml contiene: 0,3 mg de bimatoprost. Vehículo: cloreto de sódio, fosfato de sódio presentación. esentación.Frascos cuenta-gotas conteniendo 5 ml de solución oftalmológica estéril de bimatoprost a 0,03%. USO ADULTO.Composición. hepta-hidratado, ácido cítrico mono-hidratado, ácido clorídrico y/o hidróxido de sódio, cloruro de benzalconio y agua purificada qsp. Indicaciones. LUMIGAN® (bimatoprost) es indicado para la reducción de la presión intra-ocular elevada en pacientes con glaucona o hipertensión ecauciones y Adver tencias. Advertencias. Fueron relatados aumento gradual del crescimiento Contraindicaciones. LUMIGAN® (bimatoprost) está contraindicado en pacientes con hipersensibilidad al bimatoprost o cualquier otro componente de la fórmula del producto. Pr Precauciones Advertencias. ocular.Contraindicaciones. de las pestañas en el largo y espesura, y oscurecimiento de las pestañas (en 22% de los pacientes después 3 meses, y 36% después 6 meses de tratamiento), y, oscurecimiento de los párpados (en 1 a <3% de los pacientes después 3 meses y 3 a 10% de los pacientes después 6 meses de tratamiento). También fue relatado oscurecimiento del íris en 0,2% de los pacientes tratados durante 3 meses y en 1,1% de los pacientes tratados durante 6 meses. Algunas de esas alteraciones pueden ser permanentes. Pacientes que deben recibir el tratamiento ecauciones LUMIGAN® (bimatoprost) no fue estudiado en pacientes con insuficiencia renal o hepática y por lo tanto debe ser utilizado con cautela en tales pacientes.Las lentes de contacto deben de apenas uno de los ojos, deben ser informados a respecto de esas reacciones. Pr Precauciones ser retiradas antes de la instilación de LUMIGAN® (bimatoprost) y pueden ser recolocadas 15 minutos después. Los pacientes deben ser advertidos de que el producto contiene cloruro de benzalconio, que es absorvido por las lentes hidrofílicas.Si más que un medicamento de uso tópico ocular estuviera siendo utilizado, se debe respetar un intervalo de por lo menos 5 minutos entre las aplicaciones.No está previsto que LUMIGAN® (bimatoprost) presente influencia sobre la capacidad del paciente conducir vehículos u operar máquinas, sin embargo, así como para cualquier colírio, puede ocurrir visión borrosa transitoria después de la instilación; en estos casos el paciente debe aguardar que la visión se normalice antes de conducir u operar máquinas. Interacciones medicamentosas. medicamentosas.Considerando que las concentraciones circulantes sistemicas de bimatoprost son extremadamente bajas después múltiplas instilaciones oculares (menos de 0,2 ng/ml), y, que hay varias vías encimáticas envueltas en la biotransformación de bimatoprost, no son previstas interacciones medicamentosas en humanos. eacciones adversas. LUMIGAN® (bimatoprost) es bien tolerado, pudiendo causar eventos adversos oculares leves a moderados y no graves.Eventos adversos ocurriendo en 10-40% de los pacientes que recibieron doses únicas diarias, durante No son conocidas incompatibilidades. RReacciones 3 meses, en orden decreciente de incidencia fueron: hiperenia conjuntival, crecimento de las pestañas y prurito ocular.Eventos adversos ocurriendo en aproximadamente 3 a < 10% de los pacientes, en orden decreciente de incidencia, incluyeron: sequedad ocular, ardor ocular, sensación de cuerpo estraño en el ojo, dolor ocular y distúrbios de la visión.Eventos adversos ocurriendo en 1 a <3% de los pacientes fueron: cefalea, eritema de los párpados, pigmentación de la piel periocular, irritación ocular, secreción ocular, astenopia, conjuntivitis alérgica, lagrimeo, y fotofobia.En menos de 1% de los pacientes fueron relatadas: inflamación intra-ocular, mencionada como iritis y pigmentación del íris, ceratitis puntiforme superficial, alteración de las pruebas de función hepática e infecciones (principalmente resfriados e infecciones de las vías respiratorias).Con tratamientos de 6 meses de duración fueron observados, además de los eventos adversos relatados más arriba, en aproximadamente 1 a <3% de los pacientes, edema conjuntival, blefaritis y astenia. En tratamientos de asociación con betabloqueador, durante 6 meses, además de los eventos de más arriba, fueron observados en aproximadamente 1 a <3% de los pacientes, erosión de la córnea, y empeoramiento de la acuidad visual. En menos de 1% de los pacientes, blefarospasmo, depresión, retracción de los párpados, Posología y Administración. hemorragia retiniana y vértigo.La frecuencia y gravedad de los eventos adversos fueron relacionados a la dosis, y, en general, ocurrieron cuando la dosis recomendada no fue seguida.Posología Administración.Aplicar una gota en el ojo afectado, una vez al día, a la noche. La dosis no debe exceder a una dosis única diaria, pues fue demostrado que la administración más frecuente puede disminuir el efecto hipotensor sobre la hipertensión ocular.LUMIGAN® (bimatoprost) puede ser administrado concomitantemente con otros productos oftálmicos tópicos para reducir la hipertensión intra-ocular, respetándose el intervalo de por lo menos 5 minutos entre la administración de los medicamentos. VENTA BAJO PRESCRIPCIÓN MÉDICA.“ESTE PRODUCTO ES UM MEDICAMENTO NUEVO AUNQUE LAS INVESTIGACIONES HAYAN INDICADO EFICACIA Y SEGURIDAD, CUANDO CORRECTAMENTE INDICADO, PUEDEN SURGIR REACCIONES ADVERSAS NO PREVISTAS, AÚN NO DESCRIPTAS O CONOCIDAS, EN CASO DE SOSPECHA DE REACCIÓN ADVERSA, EL MÉDICO RESPONSABLE DEBE SER NOTIFICADO. 1. The AGIS Investigators: The Advanced Glaucoma Intervetion Study - The Relationship Between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophthalmol, 130 (4): 429-40, 2000. 2. Shirakashi, M. et al: Intraocular Pressure-Dependent Progression of Visual Field Loss in Advanced Primary Open-Angle Glaucoma: A 15-Year Follow-Up. Ophthalmologica, 207: 1-5, 1993. 3. Mao, LK; Stewart, WC; Shields, MB: Correlation Between Intraocular Pressure Control and Progressive Glaucomatous Damage in Primary Open-Angle Glaucoma. Am. J. Ophthalmol, 111: 51-55, 1991. 4. Higginbotham, EJ et al. One-Year Comparison of Bimatoprost with Timolol in Patients with Glaucoma or Ocular Hypertension. Presented at American Academy Ophthalmology, Nov 11-14, 2001. 5. Gandolfi, S et al. Three-Month Comparison of Bimatoprost and Latanoprost in Patients with Glaucoma and Ocular Hypertension. Adv. Ther, 18 (3): 110-121, 2001. 6. Coleman, AL et al: A 3-Month Comparison of Bimatoprost with Timolol/Dorzolamide in Patients with Glaucoma or Ocular Hypertension. Presented at American Acedemy of Ophthalmol, New Orleans, La, 2001. Mejor comodidad posológica: 1 vez al día. No requiere refrigeración. Presentación conteniendo 3 ml.