")
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/41507140
Design of a programmable multi-pattern FES system for restoring foot drop
in stroke rehabilitation
Article in Journal of Medical Engineering & Technology · February 2010
DOI: 10.3109/03091900903580496 · Source: PubMed
CITATIONS
READS
10
444
3 authors:
Sukanta Sabut
Rocky Kumar
KIIT University
Indian Institute of Technology (ISM) Dhanbad
74 PUBLICATIONS 445 CITATIONS
249 PUBLICATIONS 5,415 CITATIONS
SEE PROFILE
SEE PROFILE
Manjunatha Mahadevappa
Indian Institute of Technology Kharagpur
108 PUBLICATIONS 1,893 CITATIONS
SEE PROFILE
Some of the authors of this publication are also working on these related projects:
DWT-based Feature Extraction and Classification for Motor Imaginary EEG Signals View project
Point-of-Care healthcare delivery in emerging economies View project
All content following this page was uploaded by Sukanta Sabut on 04 April 2018.
The user has requested enhancement of the downloaded file.
Journal of Medical Engineering & Technology, Vol. 34, No. 3, April 2010, 217–223
Innovation
Design of a programmable multi-pattern FES system for restoring
foot drop in stroke rehabilitation
S. K. SABUT*{, R. KUMAR{ AND M. MAHADEVAPPA{
{School of Medical Science & Technology, Indian Institute of Technology, Kharagpur, 721302, India
{National Institute for the Orthopaedically Handicapped, Kolkata, 700090, India
(Received 20 July 2009; revised 16 December 2009; accepted 23 December 2009)
A programmable and portable multi-pattern transcutaneous neuromuscular stimulator
was developed and evaluated for correction of foot drop in stroke subjects. The
stimulator unit was designed to optimize functionality while keeping its size and power
consumption to a minimum. It had two channels of biphasic stimulation (chargebalanced and constant current), and all parameters were programmable to accommodate
a range of stimulation profiles. The ‘natural’ electromyographic (EMG) pattern of tibialis
anterior (TA) muscle stimulation envelope algorithms and constant amplitude stimulation envelope was provided for foot drop corrections in stroke patients. A foot-switch
sensor was used to trigger the device in the swing phase of gait cycle. Various tests on
prototype units were performed, including output power characteristics with a skin
model, and tested with a stroke subject to validate the results. This paper provides a
detailed description of the hardware and block-level functional electrical stimulation
(FES) system design for applications in stroke rehabilitation.
Keywords: Programmable; Neuromuscular stimulator; Electromyographic; Foot drop;
Stroke
1. Introduction
Typically, subjects who suffer a stroke lose muscular
control, affecting one side of the body, referred to as
hemiplegia [1]. Foot drop is one of the pathologies in
hemiplegic patients and refers to inadequate activation of
the dorsiflexor muscles, due to impaired selective control
and/or calf muscle spasticity [2]. The inability to properly
dorsiflex the ankle results in a dragging of the foot during
the swing phase and as a result has a significant impact on
the person’s gait.
Functional electrical stimulation (FES) is a technique
which involves the use of an electrical stimulator to correct
dropped foot in individuals who have a persistent upper
motor neurone condition [3,4]. The concept was first
proposed by Liberson in 1961, who applied a rectangular
stimulation profile to the peroneal nerve to elicit a
dorsiflexion of the foot synchronized with the swing phase
of gait to lift the foot and prevent it from dragging on the
ground during swing [5]. This stimulation profile corrected
for foot drop, which obstructs the advancing limb during
the swing phase of gait. Since Liberson’s study a number of
implanted and surface functional electrical stimulation
systems have been developed and applied successfully to
restore body functions such as standing and walking [6,7].
Lyons et al. provide a detailed review of such devices [8].
Several researchers have evaluated the effect of changes
to the stimulation intensity profile. The trapezoidal FES
intensity envelope is most commonly used in commercial
foot drop stimulators to improve the loading response
*Corresponding author. Email: [email protected]
Journal of Medical Engineering & Technology
ISSN 0309-1902 print/ISSN 1464-522X online ª 2010 Informa UK Ltd.
http://www.informaworld.com/journals
DOI: 10.3109/03091900903580496
218
S. K. Sabut et al.
phase of gait and to prevent the occurrence of foot-slap
[9,10]. Lyons et al. [11] suggested that the trapezoidal FES
envelope approach was not properly matched to the
biomechanical requirements of the tibialis anterior (TA)
muscle occurring during gait cycle and may lead to muscle
fatigue which limits the walking of the user. Vodovnik [12]
proposed adding adjustable ramp-up and ramp-down
periods to the stimulation intensity envelope to avoid rapid
contraction of the tibialis anterior and foot-flap due to
rapid shut-off of stimulus.
The work done with surface foot drop stimulators
suggests that significant improvement in orthotic performance can be achieved using stimulus intensity shapes,
which more closely match the TA activation pattern than
the trapezoidal shape currently used [13–15]. In follow-up
work, O’Keeffe et al. [16] proposed an optimized FES
stimulation intensity envelope to generate the biphasic
pattern of electromyographic (EMG) observed in the TA
during healthy gait. A more recent application of portable
neuromuscular electrical stimulation (NMES) under realtime control is for foot drop correction and blood flow
assist applications [17]. The Compex Motion stimulator
was used to develop various custom-made neuroprostheses
for physiological studies [18].
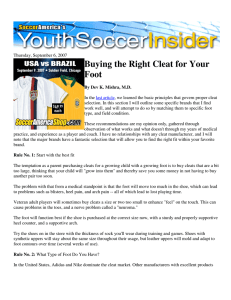
In 1977, Stanic compared the gait of two hemiplegic
subjects using a peroneal nerve stimulator (PNS) when
walking with the traditional trapezoidal stimulation profile
and when walking with a stimulation profile based on
qualitative information provided by EMG activity of a
normal person [19]. A significant improvement of the anklejoint goniograms was shown; however, no systematic
analysis of the effect of different profiles was performed.
Figure 1 shows the naturally occurring EMG activity which
will be desirable to mimic more closely the natural pattern
of the tibialis anterior muscle [20].
This study focuses on designing a low-cost, programmable neuromuscular stimulator with a stimulation profile
that more closely follows natural tibialis anterior (TA)
muscle activity in normal gait, and to investigate and
compare with constant amplitude stimulation for foot drop
correction in stroke subjects.
Figure 1. Typical activity (EMG) of the tibialis anterior
during a natural stride.
2. Neuromuscular stimulation system design
Neuroprostheses come in many different shapes and sizes,
and serve many different purposes. The three main
components required for restoring motor functions after
an injury of the central nervous system (such as poststroke) are the main unit (stimulator), sensor and surface
electrodes. The FES system was developed to exhibit
stimulus output capabilities comparable to existing neuromuscular stimulators while providing real-time stimulus
adjustment and much greater flexibility in output waveform
shape. The designed stimulator integrates the following
functionality: (1) dual channel bipolar stimulation; (2)
generation of current-controlled biphasic compensated
pulses; (3) programmability of controlled pulse width,
frequency and stimulation amplitude, with an easy-to-use
user interface; and (4) battery supply. The power to the
stimulator can be controlled by using an ON/OFF button,
and a LED indicator glows when stimulator is ON.
3. FES system
The FES device was designed to serve as a hardware
platform for development of diverse FES systems that
apply transcutaneous (surface) stimulation technology.
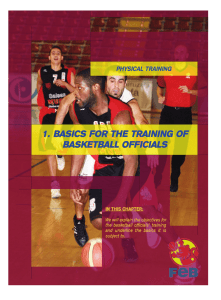
3.1. The portable stimulator unit
A functional block diagram of the portable, dual-channel
muscle stimulator unit is shown in figure 2. The stimulator
consists of four functional units: (1) microcontroller, (2)
power supply unit, (3) PC interface and (4) output stage.
The main unit consists of a microcontroller, which
generates the stimulation envelope, and a selection button
for choosing different stimulation patterns and adjusting
the stimulation parameters, which include frequency,
amplitude, and pulse width [21]. The hardware was
designed as a general platform that could be used for a
wide range of possible applications. For this purpose
analogue and digital input channels were implemented.
Basic stimulus controls were provided for each of the two
stimulation channels. Information on the operation of the
device, including the treatment time and current amplitudes, is available on the display. The stimulus intensity is
controlled externally via potentiometer. The unit acts as a
constant current generator providing biphasic output
pulses of maximum current output of 70 mA per channel.
The output stage produces the desired biphasic stimulus
waveforms by means of MOSFET switching circuitry. The
DAC080 digital to analogue converter (DAC) was used to
convert the programmed digital values into analogue values
corresponding to the output channel. The DAC0808 is an
8-bit monolithic DAC featuring a full scale output current
settling time of 150 ns while dissipating only 33 mW
with +5 V supplies. The power supply current of the
A programmable FES system for stroke rehabilitation
219
Figure 2. Block diagram of the portable FES system.
DAC0808 is independent of bit codes, and exhibits
essentially constant device characteristics over the entire
supply voltage range. Special attention was paid to the
design of the DC/DC converter, which mostly determines
the overall efficiency of the device. A modified push-pull
step-up switching converter topology was adopted as the
optimal solution. A foot switch sensor was incorporated in
the hardware design to make the stimulator ON during the
swing phase and OFF during the stance phase of walking
gait, which is usually around 60% of the gait cycle. This
ON/OFF pattern of stimulation helps to minimize muscle
fatigue by giving time for the target muscle to rest, and
extends the battery life. A 9 V rechargeable battery
provides the main power for the unit, to improve safety.
Power-saving features were incorporated in the system
design to minimize power consumption by using Complementary metal-oxide-semiconductor (CMOS) components
wherever possible. A patient-controlled cut-off button was
designed in the hardware for an emergency stop.
3.2. Microcontroller
The microcontroller is the main part of the stimulator used
for generating ‘natural’ TA muscle and periodic rectangular
pulse stimulation patterns at the desired frequency and
pulse width. It controls all of the stimulator’s functional
units (e.g. pulse generator, power supply unit and user
interface); hence many electronic components were removed from the design to reduce size and weight of the
device. After analysing the requirements for this stimulator,
220
S. K. Sabut et al.
frequency (10–50 Hz) and pulse voltage (0–120 V). In
general, the amplitude of a surface stimulation ranges from
10 to 90 mA.
4. Generated pulses
Initially two algorithms were available for foot drop and
other applications such as hand function, shoulder
subluxation and knee extension. Single or dual channel
stimulation with sensor feedback provided from the
affected leg is available for both of these algorithms. The
clinician can select a natural TA EMG envelope or
rectangular pulse patterns for treatments.
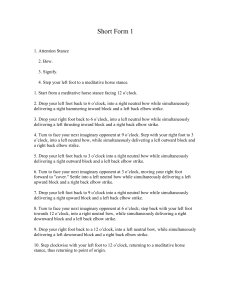
4.1. Foot drop stimulation
Figure 3. ‘Natural’ TA EMG envelope foot drop algorithm.
we chose AT89C2051 (KeilTM, an ARM1 Company) chip,
which is a low-voltage, high-performance CMOS 8-bit
microcontroller and allows changes to the program code to
be easily implemented. It provides a highly flexible and
cost-effective solution to many embedded control applications and is suitable for battery operated devices. This
microcontroller unit fulfils all requirements for newly
designed devices.
3.3. Power supply unit
The stimulator block provides two channels of stimulus
and contains a power conversion block which converts the
battery’s 9-V output to 5 V. The high voltage circuit
includes a step-up DC/DC converter to convert the 5 V
supply into the high voltage range (0–150 V) required for
stimulation in various clinical applications. Battery supplied devices are intrinsically safe and they also provide
greater mobility. A patient-controlled cut-off button was
used for an emergency stop for when painful shock
happens.
3.4. Stimulus waveform
Motor neurons can be stimulated by both monophasic and
biphasic currents or by voltage pulses. It is generally
believed that the injected charge should not be allowed to
accumulate over time as these electric charges depolarize
the membrane of the motor neuron, which causes the
generation of an action potential. Therefore, most FES
systems implement biphasic current pulses or charge
balanced waveforms, allowing the amount of the charge
to depolarize the motor neuron and then to balance the
charge. The stimulus parameters delivered by the stimulator were within the ranges used by existing muscle
stimulator devices: pulse width (100–500 ms), pulse
A ‘natural’ envelope stimulation strategy was proposed
based on muscle activation patterns observed in healthy
gait [20]. The generated stimulation waveform was close to
the natural EMG pattern of tibialis anterior muscle with a
pulse width of 250–500 ms and a stimulation frequency of
40 Hz, and applied to the driver circuit. A single cycle of
the stimulus output of 1.3 s for this algorithm, which was
adjustable (figure 3), was captured by the digital storage
oscilloscope (DSO). This natural stimulation envelope
provides tetanized muscle contraction for functional movements and reduces the charge delivered, which is a very
important for better functional performance with reduced
muscle fatigue and lower power consumption in the
electronic stimulator. This specialized stimulation envelope
could be used for the correction of foot drop in stroke and
other upper motor neuron lesions (UMNs). A foot switch
sensor control was used to control the triggering of the
stimulator; the system is ON during swing phase and OFF
during stance phase of the gait cycle.
4.2. Constant amplitude rectangular pulse
The generated stimulation pulse trains were packets of
rectangular pulses of constant current having pulse width
of 300 ms and frequency 40 Hz, which do not appear
continuously at the output, but rather in packets of bursts
with a duration of 4 s ON and 1 s OFF between successive
bursts, as shown in figure 4. This waveform pattern can
initially be used in foot drop to ensure a proper electrode
placement and for muscle conditioning.
5. System test results
To date the designed stimulator has been bench tested and
tested with healthy subjects; clinical evaluation is to follow.
This study received prior ethical approval from the
Institute Ethical Committee (IEC) and the test subjects
gave informed written consent prior to testing. Preliminary
testing of the system on subjects was promising. Further
221
A programmable FES system for stroke rehabilitation
testing will be carried out on a higher number of patients
with foot drop pathology at the clinical trial period at the
National Rehabilitation Institution. The operating specifications of the designed neurostimulator are summarized in
table 1. These electrical stimulation parameters provide
tetanized muscle contraction as required for functional
movements, and reduce the rate of fatigue within the
clinically established safety limits [17].
5.1. Testing with skin model
It was important that the stimulator should accurately
reproduce the programmed stimulation intensity parameters. The appropriate stimulus tests were performed
using a 1 kO resistor in parallel with a 100 nF capacitive
load. This was the same arrangement as used by Odstock
Medical Limited, Salisbury, UK, makers of the Odstock
Drop Foot Stimulator (ODFS). It was a simplified circuit
equivalent of the skin model and also tested with study
volunteers. The output waveforms were measured for both
tests using a Scientific SM2100 digital oscilloscope. The
accuracy of the programmable parameters for the stimulation intensity envelope was tested using a natural TA
muscle envelope and rectangular pulses. The results of the
test with a 1 kO resistor in parallel with a 100 nF capacitive
load are listed in table 2.
It was found that the performance of the muscle
stimulator matched the design conditions. As can be seen
from table 2, the stimulus output values are accurate to
within +3% of the programmed values, which satisfies the
general system requirement for accuracy. Similarly stimulus
tests were performed using a 470 O resistor in parallel with
a 100 nF capacitive load listed (table 3). The maximum
current amplitude of 72 mA, considering a load resistance
of 1 kO, was associated with the maximum peak current.
Moreover the lower percentage error in both amplitude
voltage and in the pulse width occurs for the smaller load
resistance (470 O).
5.2. Testing with subjects
The system was tested with a stroke subject walking with
the device for a 15–30-min treatment session per day over
the course of 4 weeks, and compared with the constant
amplitude rectangular stimulation pattern. The stimulation
was applied through skin-surface electrodes on the leg by
stimulating the common peroneal nerve and motor point of
the tibialis anterior muscle to produce muscle contractions
that mimic normal voluntary actions, lifting the foot off the
ground and improving gait during the swing phase. The
devices employed a heel switch to determine when the
affected limb comes into contact with the ground. When
Table 2. Stimulation intensity envelope test results.
Parameters
Pulse-width (ms)
Pulse-interval (ms)
Frequency (Hz)
Output voltage
(assuming a
1 kO load)
Range (assuming
a 1 kO load)
Voltage (V)
Amplitude (mA)
Figure 4. Packets of rectangular waves.
Features
Number of channels
Output mode
Current output
Output voltage range
Pulse width
Stimulation frequency
Battery
Characteristics
Two
Biphasic, constant-current stimulation
0–72 mA
0–120 V
300–700 ms
10–50 Hz
Rechargeable 9 V
Measured
Percentage
Error (%)
680
27.2
36.8
41
700
27.4
36.5
30
2.9
0.7
0.8
26.8
–
–
0–72
0–72
–
–
Table 3. Stimulation intensity envelope test results.
Parameters
Table 1. Specification of the stimulator.
Programmed
Pulse-width (ms)
Pulse-interval (ms)
Frequency (Hz)
Output voltage (V)
(assuming a
470O load)
Range (assuming
a 470O load)
Voltage (V)
Amplitude (mA)
Programmed
Measured
Percentage
Error (%)
680
27.2
36.8
41
680
27.4
36.5
34
0
0.7
0.8
17
–
–
0–38
0–80
–
–
222
S. K. Sabut et al.
Table 4. Temporal gait parameters and RMS values obtained from hemiplegic patients.
‘Natural TA’ pattern
Parameters
71
Speed (m s )
Cadence (steps min71)
Step length (cm)
PCI (beats m71)
Range of motion of ankle joint (active) (8)
TA muscle
RMS (mV)
Mean (mV)
Rectangular pattern
Pre-test
Post-test
% change
Pre-test
Post-test
% change
0.55
67
47
0.18
25
0.7
85
49
0.12
30
27.2
26.8
4.2
33.3
20
0.51
71
43
0.19
20
0.62
86
44
0.16
25
21.5
21.1
2.3
15.7
25
0.12
0.04
50
48.1
0.11
0.03
37.5
11.1
0.08
0.027
there is weight on the heel, the device is off. When weight is
off the heel, the device turns on, causing the ankle to
dorsiflex. At the completion of the 4-week trial, the subject
was re-evaluated for gait parameters, range of motion and
root mean square (RMS) value of EMG of tibialis anterior
muscle. Table 4 shows the compared result between
subjects tested with natural TA muscle pulse pattern and
constant rectangular pulse amplitude.
The tested result shown the walking speed increased from
0.55 ms71 to 0.7 ms71 by 27.27% with natural TA pattern
and 0.51 ms71 to 0.62 ms71 by 21.5% with constant
amplitude pattern. The RMS value of TA muscle has shown
improvement by 50% with the natural pattern and 37.5%
with the constant amplitude pattern. Similarly, other
parameters of walking gait and electromyographic activity
(table 4) showed better improvement with natural TA
pattern stimulus compared to the constant amplitude
rectangular stimulus pattern. The result indicates better
improvement in gait ability and strengthening muscle power
with natural TA pattern. The observed walking gait reveals
ankle angle trajectory closer to the normal trajectory and an
improved loading response phase, where audible foot slap
was prevented and maximal plantarflexion decreased.
5.3. Determination of strength–duration curve
We conducted an experiment to determine chronaxie/
rheobase values by plotting the strength–duration (S–D)
curves of dorsiflexor muscle. First, the rheobase was
determined at a rectangular pulse of 50 ms duration with
a stimulation frequency of 40 Hz. The S–D curve was
determined by decreasing the widths of impulses (400, 350,
300, 250, 200, 150, 100 and 50 ms), while observing a
minimal visible contraction of the muscle at that particular
amplitude (mA) of the stimulus. As the duration of a test
stimulus is increased, the strength of the current required to
just reach the stimulation threshold decreases. The S–D
characteristics of the tested subjects are shown in figure 5,
revealing that the intensity of stimulation current decreases
with increase in pulse duration for activation of muscles.
0.08
0.027
Figure 5. Average strength–duration curve (mean + SD)
(n ¼ 6).
The average normal chronaxie value of an innervated
muscle is 300 ms, after which the curve becomes saturated.
6. Discussion and conclusions
This paper describes the design, validation and evaluation
of a dual-channel microcontroller-based FES system
intended for a wide variety of clinical research settings by
replacing many of the analogue circuits. We incorporated a
‘natural’ tibialis anterior EMG muscle stimulus pattern
that could be used for clinical application in foot drop
correction, and a rectangular pattern used for common
therapeutic applications such as foot drop, hand functions
and shoulder subluxation in stroke and other neurological
disorders. The device was portable, affordable and user
friendly so that patients can carry their own FES systems to
be used at home in activities of daily living instead of
visiting hospitals regularly. Bench test evaluation showed
that the device worked satisfactorily according to designed
specifications and the efficiency of the natural stimulation
pattern was demonstrated in foot drop correction with a
hemiparetic patient. The TA muscle was stimulated and an
improvement of walking ability, and ankle joint range of
motion (ROM) and strengthened muscle power were
observed compared to the constant amplitude stimulus
A programmable FES system for stroke rehabilitation
pattern. The natural EMG pattern of the stimulus was
promising in foot drop correction with normal trajectory
ankle motion that mimics the natural gait pattern while
walking. These findings suggest that further investigation
should be carried out on larger numbers of stroke subjects
with foot drop, and also that a comparison should be made
with the conventional trapezoidal stimulation pattern.
Acknowledgements
The authors would like to acknowledge fruitful discussions
with the clinicians and application engineers of National
Institute for the Orthopaedically Handicapped, Kolkata
and Sourajit Das of the Biomedical Instrumentation
Laboratory of the School of Medical Science & Technology, IIT-Kharagpur for supporting with the development
and initial testing of the device. We would like to express
our sincere thanks to the volunteers who have taken part in
this study.
Declaration of interest: The authors report no conflicts of
interest.
[9]
[10]
[11]
[12]
[13]
[14]
[15]
References
[1] Whittle, M.W., 1996, Gait Analysis: an Introduction (Oxford: Butterworth-Heinemann).
[2] Perry, J., 1992, Gait Analysis: normal and pathological function (Slack).
New Jersey, SLACK, Inc.
[3] Taylor, P.N., 2002, The use of electrical stimulation for correction of
dropped foot in subjects with upper motor neurone lesions. Advances
in Clinical Neuroscience and Rehabilitation, 2, 16–18.
[4] Taylor, P.N., Burridge, J.H. and Dunkerley, A.L., 1999, Clinical use of
the Odstock dropped foot stimulator: its effect on the speed and effort
of walking. Archives of Physical Medicine and Rehabiliation, 80, 1577–
1583.
[5] Liberson, W.T., Holmquest, H.J., Scot, D. and Dow, M., 1961,
Functional electrotherapy: stimulation of the peroneal nerve synchronized with the swing phase of gait of hemiparetic patients. Archives of
Physical Medicine and Rehabiliation, 42, 101–105.
[6] Burridge, J., Taylor, P., Hagan, S. and Swain, I., 1997, Experience of
clinical use of the Odstock dropped foot stimulator. Artificial Organs,
21, 254–260.
[7] Guiraud, D., Stieglitz, T., Taroni, G. and Divouxet, J.L., 2006,
Original electronic design to perform epimysial and neural stimulation
in paraplegia. Neural Engineering, 3, 276–286.
[8] Lyons, G.M., Sinkjaer, T., Burridge, J.H. and Wilcox, D.J., 2002, A
review of portable FES-based neural orthoses for the correction of
View publication stats
[16]
[17]
[18]
[19]
[20]
[21]
223
drop foot. IEEE Transactions on Neural Systems and Rehabilitation
Engineering, 10, 260–279.
Burridge, J., Taylor, P., Hagan, S. and Swain, I., 1997, Experience of
clinical use of the odstock dropped foot stimulator. Artificial Organs,
21, 254–260.
Acimovic, R., Gros, N., Malezic, M., Strojnik, P., Kljajic, M., Stanic,
U. and Simic, V., 1987, A comparative study of the functionality of the
second generation of peroneal stimulators. Paper presented at the 10th
RESNA Conference. San Jose, California. Washington. DC., June 19–
23, 621–623.
Lyons, G.M., Wilcox, D.J., Lyons, D.J., et al., 2002, Evaluation of a
drop foot stimulator FES intensity envelope matched to tibialis anterior
muscle activity during walking. Proceedings of the 5th Annual Conference
on the IFESS, Aalborg, Denmark, June 18–20, pp. 448–451.
Vodovnik, L., Dimitrijevic, M.R., Prevec, T. and Logar, M., 1996,
Electronic walking aids for patients with peroneal palsy. World
Electron. Instrum, 4, 58–61.
Hart, D.J., Taylor, P.N., Chappell, P.H. and Wood, D.E., 2006, A
microcontroller system for investigating the catch effect: Functional
electrical stimulation of the common peroneal nerve. Medical
Engineering & Physics, 28, 438–448.
Stanic, U., Trnkoczy, A., Acimovic, R. and Gros, N., 1997, Effect of
gradually modulated electrical stimulation on the plasticity of
artificially evoked movements. Medical & Biological Engineering &
Computing, 15, 62–66.
O’Halloran, T., Haugland, M., Lyons, G.M. and Sinkjaer, T., 2003,
Effect of modifying stimulation profile on loading response during
FES-corrected drop foot. Paper presented at International Functional
Electrical Stimulation Society (IFESS) Conference, Queensland,
Australia.
O’Keeffe, D.T., Donnelly, A.E. and Lyons, G.M., 2003, The
development of a potential optimized stimulation intensity envelope
for drop foot applications. IEEE Transactions on Neural Systems and
Rehabilitation Engineering, 11, 249–256.
Breen, P.P., Corley, G.J., O’Keeffe, D.T. Conway, R. and O’Laighin,
G., 2009, A programmable and portable NMES device for drop foot
correction and blood flow assist applications. Medical Engineering
& Physics, 31, 400–408.
Keller, T., Popovic, M.R, Pappas, I.P. and Muller, P.Y., 2002,
Transcutaneous functional electrical stimulator ‘Compex Motion’.
Artificial Organs, 26, 219–223.
Stanic, U., Trnkoczy, A., Acimovic, R. and Gros, N., 1977, Effect of
gradually modulated electrical stimulation on the plasticity of
artificially evoked movements. Medical & Biological Engineering &
Computing, 15, 62–66.
Hart, D.J., Taylor, P.N., Chappell, P.H. and Wood, D.E., 2006, A
microcontroller system for investigating the catch effect: Functional
electrical stimulation of the common peroneal nerve. Medical
Engineering and Physics, 28, 438–448.
Cheng, K.W., Lu, Y., Tong, K.Y., Rad, A.B., Daniel and Sutanto, D.,
2004, Development of a circuit for functional electrical stimulation.
IEEE Transactions on Neural Systems and Rehabilitation Engineering,
12(1), 43–47.