request for medication to be given during school hours
Anuncio

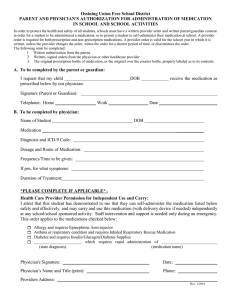
REQUEST FOR MEDICATION TO BE GIVEN DURING SCHOOL HOURS (Spanish) This request must be signed by parent/guardian and physician to authorize medication during school hours. The section in English is for the physician and the Spanish section is to be completed by parent or guardian. SCHOOL NAME: _____________________________________Fax: _______________________ TO BE COMPLETED BY PHYSICIAN: Pupil’s Name __________________________________________ Grade ________ Diagnosis ____________________________ Medication ____________________________________________ Dosage __________________________ Route ____________ Time to be given ________________________________________ Purpose of Medication ________________________________ Significant information: (include side effects and toxic reaction) __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ _________________________________________________________________________________________________________ Duration of order: From ___________________________________ to ______________________________________________ ___ Yes ___ No If medication is used for asthma/allergic reaction (ie: inhaler/epipen), I certify this student has been taught to self-administer and should be allowed to carry own medicine and use as prescribed. ____________________________________________ Physician’s Name (please print) ___________________________________________ Physician’s Signature ____________________________________________ Date ___________________________________________ Telephone Number Spanish version below signed by parent indicates the following: I request that my child be administered the medication as indicated in the physician’s order above. I understand that non-medical personnel conduct the administration. If an emergency injection is ordered, I give permission for the School Nurse to instruct designated staff in the administration technique. I understand that it is my responsibility to furnish this medication within a container properly labeled by a pharmacist with identifying information, e.g., name of child, medication dispensed, dosage prescribed and the time it is to the given and to transport the medication to school unless special arrangements are made. I authorize the release and exchange of medical and educational information between my child’s physician and school staff that is necessary in carrying out this service to my child. PARA LLENARSE POR PADRE/MADRE/TUTOR: Solicito que a mi hijo/a se le administre el medicamento como indicado en las órdenes del doctor arriba en este formulario. Comprendo que personal no-médico va administrar el medicamento. En caso de órdenes para una inyección en caso de emergencia, yo doy permiso a la Enfermera Escolar a dar instrucciones para la administración técnica al personal designado. Comprendo que es mi responsabilidad proveer el medicamento en la botella de la farmacia con información en la etiqueta indicando el nombre del niño, el medicamento, la dosis y la hora para dar el medicamento y yo soy responsable por el transporte del medicamento a la escuela a menos que se hacen arreglos especiales. Yo autorizo el intercambio de información médica y educativa que sea necesario entre el doctor y el personal escolar para llevar a cabo este servicio para mi hijo/a. ____________________________________ Firma de Padre/Madre/Tutor _____________________________ # de Teléfono/Celular Health-Request for Medication during School Hours Revised 06-2010 _______________________ Fecha