Appl for Emer Absentee Ballot Due to Death in Family [5/88]
Anuncio

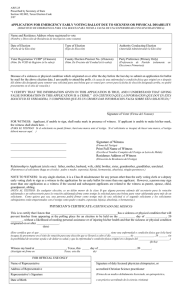
Name of Form: Application for Emergency Ballot Due to Death in Family. Section Reference: Section 103.002, Texas Election Code. Purpose: To allow a voter to vote who will be absent from the county of residence on election day because of a death that occurs on or after the day before the last day of the period for early voting by personal appearance. The voter must be related within the second degree of consanguinity or affinity to the deceased person. Number of Copies Required: One. Completed by: The Voter; Early Voting Clerk administers oath. Filing Date: On or after the 3rd day before election day and before the close of business the day before the election. Filed with: Early Voting Clerk, in person. Comments: 1. This form incorporates an application to vote early with an affidavit qualifying the voter to vote by this procedure. 2. The affidavit on the carrier envelope need not be completed when a voter is voting under this procedure. The early voting clerk shall, however, make a notation "Late ballot due to death" on the carrier envelope. 3. This special provision for voting a late ballot is conducted with the balloting materials for voting by mail. Current form is 3/07. 5-24 AW5-24 Prescribed by Secretary of State Section 103.002, Texas Election Code 3/07 APPLICATION FOR EMERGENCY EARLY BALLOT DUE TO DEATH IN FAMILY (SOLICITUD DE EMERGENCIA PARA UNA BOLETA PARA VOTAR ADELANTADA A CAUSA DE LA MUERTE DE UN MIEMBRO DE LA FAMILIA) Name and Residence Address where registered to vote (Nombre y Dirección de Residencia de inscripcion como votante) Date of Election Type of Election Authority Conducting Election (Fecha de la Elección) (Tipo de Elección) (Autoridad Administrando la Elección) Voter Registration VUID* (if known County Election Precinct No. (if known) Party Preference (Primary Only) (Núm. De VUID de Registro (si lo sabe)) (Núm. De Precinto del Condad (si lo sabe)) (Preferencia de Partido Elecciones Primarias)) (solamente en “I CERTIFY THAT THE INFORMATION GIVEN IN THIS APPLICATION IS TRUE, AND I UNDERSTAND THAT GIVING FALSE INFORMATION IN THIS APPLICATION IS A CRIME.” (YO CERTIFICO QUE LA INFORMACION QUE DOY EN ESTA SOLICITUD ES VERDADERA, Y COMPRENDO QUE ES UN CRIMEN DAR INFORMACION FALSA SOBRE ESTA SOLICITUD.)” ____________________________________ Signature of Voter (Firma del Votante) FOR WITNESS: Applicant, if unable to sign, shall make mark in presence of witness. If applicant is unable to make his/her mark, the witness shall check here. (PARA EL TESTIGO: Si el solicitante no puede firmar, hará una marca ante el testigo. Si el solicitante es incapaz de hacer una marca, el testigo deberá marcar aguí. ) __________________________________ Signature of Witness (Firma del Testigo) __________________________________ Print Full Name of Witness __________________________________ Residence Address of Witness (Escriba el Nombre Completo del Testigo en Letra de Molde) (Dirección de Residencia del Testigo) Relationship to Applicant (circle one): father, mother, husband, wife, child, brother, sister, grandmother, grandfather, unrelated. (Parentresco al solicitante (haga un círculo): padre o madre, esposo(a), hijo(a), hermano(a), abuelo(a), ningún parentesco.) NOTE TO WITNESS: In any single election, it is a Class B misdemeanor for any person other than the early voting clerk or a deputy early voting clerk to sign as a witness to the application for a ballot for more than one applicant. However, a person may sign more than one application as a witness if the second and subsequent applicants are related to the witness as parent, spouse, child, grandparent, sibling. (NOTA AL TESTIGO: En cualquier elección, es un delito menor de la clase B que alguna persona además del secretario para la votación adelantada o un subsecretario para la votación adelantada firma como testigo la solicitud para una boleta para votar adelantada para más de un solicitante. Como quiera que sea, una persona podrá firmar como testigo más de una solicitud si el segundo solicitante y los solicitantes subsiguientes están emparentados con el testigo como padre o madre, esposo(a), hijo(a), abuelo(a), o hermano(a).) AFFIDAVIT (DECLARACION JURADA) I, ________________________________________________, do hereby swear or affirm that due to the death (Yo, (name of voter) (nombre del votante) por la presente juro o afirmo que a causa de la muerte of my _____________________________, which occurred on _________________, I will be absent from the county de mi (relationship of decedent) (parentesco al votante) que sucedió (date of death) (fecha de muerte) estaré fuera del condado on election day. el día de elección.) ____________________________________ Signature of Voter(Firma del Votante) Sworn to and subscribed before me, this ______ day of ________________________, 20 _______. Jurado y suscrito ante mí, este día de ____________________________________ Signature of officer administering oath (Firma del oficial administrando el juramento) Name of Form: Application for Emergency Early Voting Ballot Due to Sickness or Physical Disability. Section Reference: Section 102.002, Texas Election Code. Purpose: To allow a voter who, because of sickness or physical disability originating on or after the day before the last day to submit an application for ballot by mail, will be unable to attend the polling place on election day, to vote early under this procedure. Number of Copies Required: One. Completed by: The Voter and Physician. Filing Date: On or after the 3rd day before election and no later than 5:00 p.m. on election day. Filed with: Early Voting Clerk. Comments: 1. See Section 102.003(c) for eligibility requirements of an applicant's representative. 2. The same representative who delivered application must also deliver carrier envelope. 3. The deadline for returning a marked ballot is 7:00 p.m. on election day. 4. The early voting clerk enters the representative's name and residence address on a returned carrier envelope and secures representative's signature on the carrier envelope. 5. The voting of a late ballot under this procedure is in the same manner as an early voting ballot by mail. Current form is 3/07. 5-25 AW5-25 Prescribed by Secretary of State Section 102.002, Texas Election Code 3/07 APPLICATION FOR EMERGENCY EARLY VOTING BALLOT DUE TO SICKNESS OR PHYSICAL DISABILITY (SOLICITUD DE EMERGENCIA PARA UNA BOLETA PARA VOTAR A CAUSA DE UNA ENFERMEDAD O INCAPACIDAD FISICA) Name and Residence Address where registered to vote (Nombre y Dirección de Residencia de inscripcion como votante) Date of Election Type of Election Authority Conducting Election (Fecha de la Elección) (Tipo de Elección) (Autoridad Administrando la Elección) Voter Registration VUID* (if known) County Election Precinct No. (if known) Party Preference (Primary Only) (Núm. De VUID de Registro (si lo sabe)) (Núm. De Precinto del Condad (si lo sabe)) (Preferencia de Partido Elecciones Primarias)) (solamente en Because of a sickness or physical condition which originated on or after the day before the last day to submit an application for ballot by mail for the above election date, I am unable to attend the polls. (A causa de una enfermedad o condición física que originó en o después del ultimo día designado para someter una solicitud para una boleta que se votará por correo para la fecha de elección designada arriba, no podré presentarme en el sitio de votación.) “I CERTIFY THAT THE INFORMATION GIVEN IN THIS APPLICATION IS TRUE, AND I UNDERSTAND THAT GIVING FALSE INFORMATION IN THIS APPLICATION IS A CRIME.” (YO CERTIFICO QUE LA INFORMACION QUE DOY EN ESTA SOLICITUD ES VERDADERA, Y COMPRENDO QUE ES UN CRIMEN DAR INFORMACION FALSA SOBRE ESTA SOLICITUD.)” ____________________________________ Signature of Voter (Firma del Votante) FOR WITNESS: Applicant, if unable to sign, shall make mark in presence of witness. If applicant is unable to make his/her mark, the witness shall check here. (PARA EL TESTIGO: Si el solicitante no puede firmar, hará una marca ante el testigo. Si el solicitante es incapaz de hacer una marca, el testigo deberá marcar aquí. ) __________________________________ Signature of Witness (Firma del Testigo) __________________________________ Print Full Name of Witness __________________________________ Residence Address of Witness (Escriba el Nombre Completo del Testigo en Letra de Molde) (Dirección de Residencia del Testigo) Relationship to Applicant (circle one): father, mother, husband, wife, child, brother, sister, grandmother, grandfather, unrelated. (Parentresco al solicitante (haga un círculo): padre o madre, esposo(a), hijo(a), hermano(a), abuelo(a), ningún parentesco.) NOTE TO WITNESS: In any single election, it is a Class B misdemeanor for any person other than the early voting clerk or a deputy early voting clerk to sign as a witness to the application for an early ballot for more than one applicant. However, a person may sign more than one application as a witness if the second and subsequent applicants are related to the witness as parent, spouse, child, grandparent, sibling. (NOTA AL TESTIGO: En cualquier elección, es un delito menor de la clase B que alguna persona además del secretario para la votación adelantada o un subsecretario para la votación adelantada firma como testigo la solicitud para una boleta para votar adelantada para más de un solicitante. Como quiera que sea, una persona podrá firmar como testigo más de una solicitud si el segundo solicitante y los solicitantes subsiguientes están emparentados con el testigo como padre o madre, esposo(a), hijo(a), abuelo(a), o hermano(a).) PHYSICIAN’S CERTIFICATE (CERTIFICADO DEL MEDICO) This is to certify that I know that _____________________________________________has a sickness or physical condition that will prevent him/her from appearing at the polling place for an election to be held on the ___________ day of ______________, 20 ________, without a likelihood of needing personal assistance or of injuring his/her health and that the sickness or physical condition originated on or after _______________. (date) (Esto certifica que sé que _____________________________________________________ tiene una enfermedad o condición fisica que lo/la hará incapaz de presentarse en el sitio de votación para una elección que se llevará a cabo el día ______________ de _______________, 20 ______, sin la posibilidad de necesitar ayuda o de dañar su salud, y que la enfermedad o condición fisica originó en o después del _______________________.) (fecha) Witness my hand at _____________________, Texas, this _____ day of _________________________, 20 _______. (Atestigúe mi firma en Texas, este día de) FOR OFFICIAL USE ONLY Name of Representative Signature of duly licensed physician chiropractor, or Address of Representative accredited Christian Science practitioner Representative’s Signature (Firma de un medico debidamente licenciado, un quiropráctico, Date of Birth o un práctico acreditado de la ciencia cristiana)
![Appl for Emer Absentee Ballot Due to Death in Family [5/88]](http://s2.studylib.es/store/data/005013588_1-e472556746d500bf5e47b3e55e6cbc9b-300x300.png)